Learning Outcome
- List the causes of hypothyroidism
- Describe the clinical features of hypothyroidism
- Summarize the treatment of hypothyroidism
- Recall the nursing management plans for hypothyroidism
The thyroid gland in the anterior neck secretes thyroid hormones and is essential for multiple metabolic functions spanning almost every organ system. Hypothyroidism results from low levels of thyroid hormone. However, the etiology and manifestations of hypothyroidism are varied. Clinicians treat hypothyroidism with levothyroxine. Untreated hypothyroidism increases morbidity and mortality. This article reviews hypothyroidism's etiology, clinical presentation, diagnosis, and management.
The most common etiology is iodine deficiency in iodine-deficient geographic areas worldwide. Autoimmune thyroid diseases are the leading cause of hypothyroidism in the US and the iodine-sufficient regions. Etiology can be influenced locally by iodine fortification and the emergence of new iodine-deficient areas.[1]
Other common causes of hypothyroidism are drugs such as amiodarone and lithium, thyroid radioactive iodine therapy or thyroid surgery, radiotherapy to the head or neck area, and central hypothyroidism from neoplastic, infiltrative, inflammatory, or iatrogenic disorders of the pituitary or hypothalamus.[2][1][2]
The National Health and Nutrition Examination Survey (NHANESIII) study found the prevalence of overt hypothyroidism among US adults aged 12 years and older to be 0.3% and subclinical hypothyroidism 4.3%. Female gender and increasing age were associated with higher thyroid-stimulating hormone (TSH) and prevalence of antithyroid antibodies.[3]
A high index of suspicion should be maintained for hypothyroidism since the signs and symptoms can be mild and nonspecific, and different symptoms may be present in other patients.
Inquire about dry skin, voice changes, hair loss, constipation, fatigue, muscle cramps, cold intolerance, sleep disturbances, menstrual cycle abnormalities, weight gain, and galactorrhea.[2] Also, obtain a complete medical, surgical, medication, and family history. History of adverse pregnancy and neonatal outcomes should also be sought.[4]
Symptoms of depression, anxiety, psychosis, and cognitive impairments (eg, memory loss) can be present.[5] Rarely patients can present with ascites, rhabdomyolysis, and pericardial effusion.[6][7][6]
Patients can also present with carpal tunnel syndrome, sleep apnea, hyponatremia, hypercholesterolemia, congestive heart failure, and prolonged QT interval.[2]
A physical examination may reveal an enlarged thyroid gland, nodules, prolonged ankle reflex relaxation time, hoarse voice, and skin and hair changes.[2]
Serum TSH level is used to screen for primary hypothyroidism in most patients. In overt hypothyroidism, TSH levels are elevated, and free T4 levels are low. In subclinical hypothyroidism, TSH levels are elevated, and free T4 levels are normal.[2]
Central hypothyroidism is of pituitary or hypothalamic origin. The TSH produced can be biologically inactive and affect the levels of bioactive TSH; hence, the diagnosis of central hypothyroidism should be based on free T4 rather than TSH.[2]
Labs should include evaluation for autoimmune thyroid diseases with levels of anti-thyroid antibodies: the thyroid peroxidase antibodies and anti-thyroglobulin antibodies. Particularly in patients with thyroid nodules, fine-needle aspiration biopsy should be considered.[2]
Patients with subclinical hypothyroidism and thyroid peroxidase antibody positivity have a greater risk of developing overt hypothyroidism. These patients should be followed up periodically with clinical evaluation and lab tests. T3 levels are not a reliable or recommended test.[2] Hospitalized patients should undergo TSH testing only when thyroid dysfunction is suspected.[2] On labs, hyperlipidemia, elevated serum CK, elevated hepatic enzymes, and anemia can be present.[2] BUN, creatinine, and uric acid levels can also be elevated.[8]
Hypothyroidism is primarily treated with levothyroxine monotherapy.[9] The replacement levothyroxine dosage should be between 1.6 to 1.8 mcg/kg by mouth daily.[10] However, in patients who are older or with atrial fibrillation, reduction of the dose or starting at a low dosage and titrating up slowly as needed is essential.[9]
When switching to the intravenous (IV) form, reduce the dose to 70% of the oral dose. Malabsorption syndromes, medications such as sucralfate, calcium preparations, and bile acid sequestrants can interfere with the absorption of levothyroxine.[2]
Based on the 2012 Clinical Practice Guidelines for Hypothyroidism in Adults by the American Association of Clinical Endocrinologists and the American Thyroid Association, therapy should be monitored and titrated based on serum TSH or free T4 measurements. Laboratory studies should be drawn every 4 to 8 weeks until target levels are achieved. Laboratory measurements should also be performed after starting treatment, after any dose change, after any change in the formulation or brand of levothyroxine, and after starting or stopping any medications that may affect the thyroid hormone levels.[2] If thyroid hormone levels are stable, then the monitoring interval can be extended to 6 months; if levels remain stable, then monitoring can be further extended to 12 months or done at shorter intervals on an individualized basis along with clinical evaluation.[2] Central hypothyroidism should be monitored based on free T4 rather than TSH.[2] For elderly patients and patients with cardiac diseases, starting at a lower dose and titrating slowly is recommended.[9]Patients with cardiac disease should be monitored for the development of any symptoms of angina and atrial fibrillation.[2] If a patient is overly treated with thyroid replacement for an extended period, screening for osteoporosis is warranted.[9]
Effective treatment should achieve a clinical improvement of signs and symptoms, along with an improved sense of patient well-being and normal TSH or free T4 levels.[11] A comprehensive differential diagnosis workup is recommended for unresolved symptoms in the presence of biochemical euthyroidism. There is a lack of strong evidence supporting the routine inclusion of triiodothyronine (T3) preparations with levothyroxine in the treatment of hypothyroidism.[12]
If symptoms persist despite normalization of TSH/free T4 levels, then consultation with an endocrinologist should also be considered. Thyroid replacement treatment can exacerbate coexisting adrenal insufficiency. Patients with known or suspected adrenal insufficiency should be tested and treated for the adrenal insufficiency while awaiting results.[2] Adrenal insufficiency can also be associated with subclinical hypothyroidism that is reversible with the treatment of adrenal insufficiency.[13] In patients who have confirmed adrenal insufficiency, consider a reassessment of thyroid tests following adequate treatment of adrenal insufficiency.
Monitor for signs and symptoms of overtreatment with levothyroxine. Indications of overtreatment mimic signs and symptoms of hyperthyroidism, such as anxiety, palpitations, tachycardia, heat intolerance, fever, excessive sweating, changes in appetite, and weight loss. Report any signs of cardiac excitability, chest pain, and dysrhythmias to the medical provider.
Hypothyroidism affects multiple organ systems across all age groups and affects patient well-being and ability to function daily. Treatment is with levothyroxine monotherapy.[2] Effective treatment calls for a team-based and patient-centered approach. An endocrinology consult should be obtained when patient symptoms are not adequately controlled.
Endocrinology consultation is also recommended in complex scenarios such as preconception, pregnancy, congenital and pediatric hypothyroidism, failure of treatment, co-existing cardiac or other endocrine disorders, difficulty in interpretation of thyroid test results, and drug-induced hypothyroidism.[2] Other specialists that may be needed are a psychiatrist, obstetrician-gynecologist, pediatrician, cardiologist, and intensivist.
Pharmacists help provide advice on medication and food interactions, the effect of changes in levothyroxine formulations, and investigating the causes for the requirement of unusually high doses of levothyroxine or fluctuating TSH levels. Prompt notification to physicians of unusually high levels of TSH by laboratory personnel and close monitoring of vital signs and mental status by nurses can facilitate early treatment and better outcomes, especially in the inpatient setting (eg, myxedema coma). Rapid response teams can be effectively utilized when severe long-term hypothyroidism causes hemodynamic instability from myxedema coma. Close interprofessional communication with all the involved teams is essential to improve patient outcomes.
Advise patients that treatment for hypothyroidism is lifelong. Instruct clients to take medications 30 to 60 minutes before the first meal of the day is essential. Also, inform patients not to take thyroid medications with other medications, as several food and medication interactions may occur.
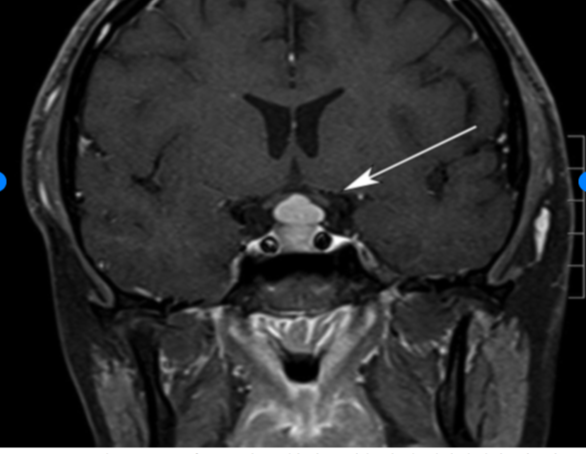
Pituitary Hyperplasia. The hyperplasia is due to primary hypothyroidism.
Siddiqi AI, Grieve J, Baldeweg SE, Miszkiel K. Tablets or scalpel: pituitary hyperplasia due to primary hypothyroidism. Radiol Case Rep. 2016;10(2):1099. doi: 10.2484/rcr.v10i2.1099.
Taylor PN, Albrecht D, Scholz A, Gutierrez-Buey G, Lazarus JH, Dayan CM, Okosieme OE. Global epidemiology of hyperthyroidism and hypothyroidism. Nature reviews. Endocrinology. 2018 May:14(5):301-316. doi: 10.1038/nrendo.2018.18. Epub 2018 Mar 23 [PubMed PMID: 29569622]
Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, Pessah-Pollack R, Singer PA, Woeber KA, American Association Of Clinical Endocrinologists And American Thyroid Association Taskforce On Hypothyroidism In Adults. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid : official journal of the American Thyroid Association. 2012 Dec:22(12):1200-35. doi: 10.1089/thy.2012.0205. Epub 2012 Nov 6 [PubMed PMID: 22954017]
Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM, American Thyroid Association Task Force on Thyroid Hormone Replacement. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid : official journal of the American Thyroid Association. 2014 Dec:24(12):1670-751. doi: 10.1089/thy.2014.0028. Epub [PubMed PMID: 25266247]
Peng CC, Pearce EN. An update on thyroid disorders in the postpartum period. Journal of endocrinological investigation. 2022 Aug:45(8):1497-1506. doi: 10.1007/s40618-022-01762-1. Epub 2022 Feb 18 [PubMed PMID: 35181848]
Phowira J, Coffey KL, Bartholomew PH, Vennart N, Moreira M, Emerson H, Kennedy D, Weaver JU. Radioactive Iodine for the Treatment of Subclinical Thyrotoxicosis Grade 1 and 2: Outcome of up to 18-Year Follow Up. Frontiers in endocrinology. 2022:13():843857. doi: 10.3389/fendo.2022.843857. Epub 2022 Mar 9 [PubMed PMID: 35370990]
Xing YZ, Zhang K, Jin G. Predictive factors for the outcomes of Graves' disease patients with radioactive iodine (131I) treatment. Bioscience reports. 2020 Jan 31:40(1):. doi: 10.1042/BSR20191609. Epub [PubMed PMID: 31840740]
Paparella R, Menghi M, Micangeli G, Leonardi L, Profeta G, Tarani F, Petrella C, Ferraguti G, Fiore M, Tarani L. Autoimmune Polyendocrine Syndromes in the Pediatric Age. Children (Basel, Switzerland). 2023 Mar 19:10(3):. doi: 10.3390/children10030588. Epub 2023 Mar 19 [PubMed PMID: 36980146]
Bjørklund G, Pivin M, Hangan T, Yurkovskaya O, Pivina L. Autoimmune polyendocrine syndrome type 1: Clinical manifestations, pathogenetic features, and management approach. Autoimmunity reviews. 2022 Aug:21(8):103135. doi: 10.1016/j.autrev.2022.103135. Epub 2022 Jun 9 [PubMed PMID: 35690244]
Burch HB. Drug Effects on the Thyroid. The New England journal of medicine. 2019 Aug 22:381(8):749-761. doi: 10.1056/NEJMra1901214. Epub [PubMed PMID: 31433922]
El Sabbagh R, Azar NS, Eid AA, Azar ST. Thyroid Dysfunctions Due to Immune Checkpoint Inhibitors: A Review. International journal of general medicine. 2020:13():1003-1009. doi: 10.2147/IJGM.S261433. Epub 2020 Nov 4 [PubMed PMID: 33177863]
Muir CA, Clifton-Bligh RJ, Long GV, Scolyer RA, Lo SN, Carlino MS, Tsang VHM, Menzies AM. Thyroid Immune-related Adverse Events Following Immune Checkpoint Inhibitor Treatment. The Journal of clinical endocrinology and metabolism. 2021 Aug 18:106(9):e3704-e3713. doi: 10.1210/clinem/dgab263. Epub [PubMed PMID: 33878162]
Pappa T, Refetoff S. Resistance to Thyroid Hormone Beta: A Focused Review. Frontiers in endocrinology. 2021:12():656551. doi: 10.3389/fendo.2021.656551. Epub 2021 Mar 31 [PubMed PMID: 33868182]
Ju JS, Cui T, Zhao J, Chen JL, Ju HB. Clinical presentation and magnetic resonance imaging characteristics of lymphocytic hypophysitis: a systematic review with meta-analysis. Archives of medical science : AMS. 2023:19(4):976-986. doi: 10.5114/aoms/144628. Epub 2021 Dec 14 [PubMed PMID: 37560735]
Khoury T, Kadah A, Mari A, Sbeit W, Drori A, Mahamid M. Thyroid Dysfunction is Prevalent in Autoimmune Hepatitis: A Case Control Study. The Israel Medical Association journal : IMAJ. 2020 Feb:22(2):100-103 [PubMed PMID: 32043327]
Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). The Journal of clinical endocrinology and metabolism. 2002 Feb:87(2):489-99 [PubMed PMID: 11836274]
Feldt-Rasmussen U, Effraimidis G, Klose M. The hypothalamus-pituitary-thyroid (HPT)-axis and its role in physiology and pathophysiology of other hypothalamus-pituitary functions. Molecular and cellular endocrinology. 2021 Apr 5:525():111173. doi: 10.1016/j.mce.2021.111173. Epub 2021 Feb 4 [PubMed PMID: 33549603]
Anand A, Singh KR, Kushwaha JK, Hussain N, Sonkar AA. Papillary Thyroid Cancer and Hashimoto's Thyroiditis: An Association Less Understood. Indian journal of surgical oncology. 2014 Sep:5(3):199-204. doi: 10.1007/s13193-014-0325-4. Epub 2014 Jul 4 [PubMed PMID: 25419066]
Hou J, Yu P, Zhu H, Pan H, Li N, Yang H, Jiang Y, Wang L, Wang B, Wang Y, You L, Chen S. The impact of maternal hypothyroidism during pregnancy on neonatal outcomes: a systematic review and meta-analysis. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology. 2016:32(1):9-13. doi: 10.3109/09513590.2015.1104296. Epub 2015 Nov 3 [PubMed PMID: 26527131]
Samuels MH. Psychiatric and cognitive manifestations of hypothyroidism. Current opinion in endocrinology, diabetes, and obesity. 2014 Oct:21(5):377-83. doi: 10.1097/MED.0000000000000089. Epub [PubMed PMID: 25122491]
Zare-Khormizi MR, Rahmanian M, Pourrajab F, Akbarnia S. Massive pericardial effusion and rhabdomyolysis secondary to untreated severe hypothyroidism: the first report. Acta clinica Belgica. 2014 Oct:69(5):375-8. doi: 10.1179/2295333714Y.0000000049. Epub 2014 Jul 24 [PubMed PMID: 25056490]
Khalid S, Asad-Ur-Rahman F, Abbass A, Gordon D, Abusaada K. Myxedema Ascites: A Rare Presentation of Uncontrolled Hypothyroidism. Cureus. 2016 Dec 5:8(12):e912. doi: 10.7759/cureus.912. Epub 2016 Dec 5 [PubMed PMID: 28083456]
Saini V, Yadav A, Arora MK, Arora S, Singh R, Bhattacharjee J. Correlation of creatinine with TSH levels in overt hypothyroidism - a requirement for monitoring of renal function in hypothyroid patients? Clinical biochemistry. 2012 Feb:45(3):212-4. doi: 10.1016/j.clinbiochem.2011.10.012. Epub 2011 Oct 28 [PubMed PMID: 22061337]
Jonklaas J. Optimal Thyroid Hormone Replacement. Endocrine reviews. 2022 Mar 9:43(2):366-404. doi: 10.1210/endrev/bnab031. Epub [PubMed PMID: 34543420]
Barlow BT, Roberts RJ, Newman K, Harrison SK, Sin JH. Economic Evaluation of a Pharmacist-Led 5-Day Therapeutic Hold of IV Levothyroxine at an Academic Medical Center. Hospital pharmacy. 2022 Feb:57(1):20-25. doi: 10.1177/0018578720970457. Epub 2020 Nov 9 [PubMed PMID: 35521003]
Antonelli A, Elia G, Ragusa F, Paparo SR, Cavallini G, Benvenga S, Ferrari SM, Fallahi P. The Stability of TSH, and Thyroid Hormones, in Patients Treated With Tablet, or Liquid Levo-Thyroxine. Frontiers in endocrinology. 2021:12():633587. doi: 10.3389/fendo.2021.633587. Epub 2021 Mar 10 [PubMed PMID: 33790863]
Trimboli P, Scappaticcio L, De Bellis A, Maiorino MI, Knappe L, Esposito K, Bellastella G, Giovanella L. Different Formulations of Levothyroxine for Treating Hypothyroidism: A Real-Life Study. International journal of endocrinology. 2020:2020():4524759. doi: 10.1155/2020/4524759. Epub 2020 Jan 20 [PubMed PMID: 32184819]
Laurent I, Tang S, Astère M, Wang KR, Deng S, Xiao L, Li QF. Liquid L-thyroxine versus tablet L-thyroxine in patients on L- thyroxine replacement or suppressive therapy: a meta-analysis. Endocrine. 2018 Jul:61(1):28-35. doi: 10.1007/s12020-018-1574-8. Epub 2018 Mar 23 [PubMed PMID: 29572710]
Trimboli P, Virili C, Centanni M, Giovanella L. Thyroxine Treatment With Softgel Capsule Formulation: Usefulness in Hypothyroid Patients Without Malabsorption. Frontiers in endocrinology. 2018:9():118. doi: 10.3389/fendo.2018.00118. Epub 2018 Mar 21 [PubMed PMID: 29619010]
Cappelli C, Negro R, Pirola I, Gandossi E, Agosti B, Castellano M. Levothyroxine liquid solution versus tablet form for replacement treatment in pregnant women. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology. 2016:32(4):290-2. doi: 10.3109/09513590.2015.1113518. Epub 2015 Nov 20 [PubMed PMID: 26585420]
Benvenga S. Liquid and softgel capsules of l-thyroxine results lower serum thyrotropin levels more than tablet formulations in hypothyroid patients. Journal of clinical & translational endocrinology. 2019 Dec:18():100204. doi: 10.1016/j.jcte.2019.100204. Epub 2019 Aug 6 [PubMed PMID: 31844631]
Gonzales KM, Stan MN, Morris JC 3rd, Bernet V, Castro MR. The Levothyroxine Absorption Test: A Four-Year Experience (2015-2018) at The Mayo Clinic. Thyroid : official journal of the American Thyroid Association. 2019 Dec:29(12):1734-1742. doi: 10.1089/thy.2019.0256. Epub 2019 Dec 4 [PubMed PMID: 31680654]
Ghosh S, Pramanik S, Biswas K, Bhattacharjee K, Sarkar R, Chowdhury S, Mukhopadhyay P. Levothyroxine Absorption Test to Differentiate Pseudomalabsorption from True Malabsorption. European thyroid journal. 2020 Jan:9(1):19-24. doi: 10.1159/000504218. Epub 2019 Nov 20 [PubMed PMID: 32071898]
Caron P, Declèves X. The Use of Levothyroxine Absorption Tests in Clinical Practice. The Journal of clinical endocrinology and metabolism. 2023 Jul 14:108(8):1875-1888. doi: 10.1210/clinem/dgad132. Epub [PubMed PMID: 36916146]
Ettleson MD, Bianco AC. Individualized Therapy for Hypothyroidism: Is T4 Enough for Everyone? The Journal of clinical endocrinology and metabolism. 2020 Sep 1:105(9):e3090-104. doi: 10.1210/clinem/dgaa430. Epub [PubMed PMID: 32614450]
Hennessey JV, Espaillat R. Current evidence for the treatment of hypothyroidism with levothyroxine/levotriiodothyronine combination therapy versus levothyroxine monotherapy. International journal of clinical practice. 2018 Feb:72(2):. doi: 10.1111/ijcp.13062. Epub 2018 Jan 30 [PubMed PMID: 29381251]
Guglielmi R, Frasoldati A, Zini M, Grimaldi F, Gharib H, Garber JR, Papini E. ITALIAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS STATEMENT-REPLACEMENT THERAPY FOR PRIMARY HYPOTHYROIDISM: A BRIEF GUIDE FOR CLINICAL PRACTICE. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2016 Nov:22(11):1319-1326 [PubMed PMID: 27482609]
Abdullatif HD, Ashraf AP. Reversible subclinical hypothyroidism in the presence of adrenal insufficiency. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2006 Sep-Oct:12(5):572 [PubMed PMID: 17002934]
Mathew V, Misgar RA, Ghosh S, Mukhopadhyay P, Roychowdhury P, Pandit K, Mukhopadhyay S, Chowdhury S. Myxedema coma: a new look into an old crisis. Journal of thyroid research. 2011:2011():493462. doi: 10.4061/2011/493462. Epub 2011 Sep 15 [PubMed PMID: 21941682]