Continuing Education Activity
Gastric ultrasound is performed to evaluate stomach contents prior to induction of anesthesia. This information allows practitioners to proactively manage the risk of aspiration of gastric contents. Information obtained from gastric ultrasound enables anesthesia providers to determine the optimal timing of procedures, type of anesthesia, and airway management technique. This activity reviews gastric ultrasound and highlights the role of the interprofessional team in evaluating gastric contents for patients undergoing procedures requiring sedation or anesthesia.
Objectives:
- Review the anatomy of the stomach and adjacent organs.
- Describe the necessary equipment and the proper technique to perform a gastric ultrasound exam.
- Describe the imaging findings associated with an empty stomach, liquid in the stomach, and solid food in the stomach.
- Summarize the findings of gastric ultrasound and how they can be used to determine the risk of pulmonary aspiration of gastric contents.
Introduction
Aspiration of gastric contents is a common cause of perioperative morbidity and mortality. Aspiration can lead to hypoxia, bronchospasm, pneumonitis, pneumonia, acute respiratory distress syndrome, and death. Aspiration pneumonia among surgical patients is associated with a 4.0-fold increased risk of intensive care admission, a 9-day increase in length of stay, and a 7.6-fold increased risk of in-hospital mortality.[1] The presence of food or liquids in the stomach before the induction of anesthesia is one of the greatest risk factors for perioperative pulmonary aspiration.[2][3][4]
The risk of gastric aspiration can be reduced by fasting before planned procedures. The American Society for Anesthesiologists Practice Guidelines for Preoperative Fasting is intended to reduce gastric aspiration risk. These guidelines recommend that healthy patients fast for a minimum of 2 hours for clear liquids; 4 hours for human breastmilk; 6 hours for non-human breastmilk, infant formula, or light meals; and 8 hours for fried foods, fatty foods, and meat.[5][6]
No clear guidance on appropriate fasting periods is provided for patients at increased risk of delayed gastric emptying or pulmonary aspiration, such as those with diabetes mellitus, gastroesophageal reflux disease, morbid obesity pregnancy, or recent opioid use. Providers also face the challenge of unclear NPO status, as seen in poor historians, patients with dementia, language barriers, and non-compliant patients.[7][8][9]
Gastric ultrasound is a simple, fast, non-invasive bedside diagnostic test that provides a qualitative and quantitative assessment of gastric contents.[10][2] The use of gastric ultrasound allows anesthesia providers to differentiate between the full and empty stomach, determine the consistency of gastric contents (solids, thick liquids, clear liquids), and estimate the volume of gastric fluids. This information is used to determine the most appropriate timing for elective procedures, anesthetic choice, and airway management approach.[11]
Anatomy and Physiology
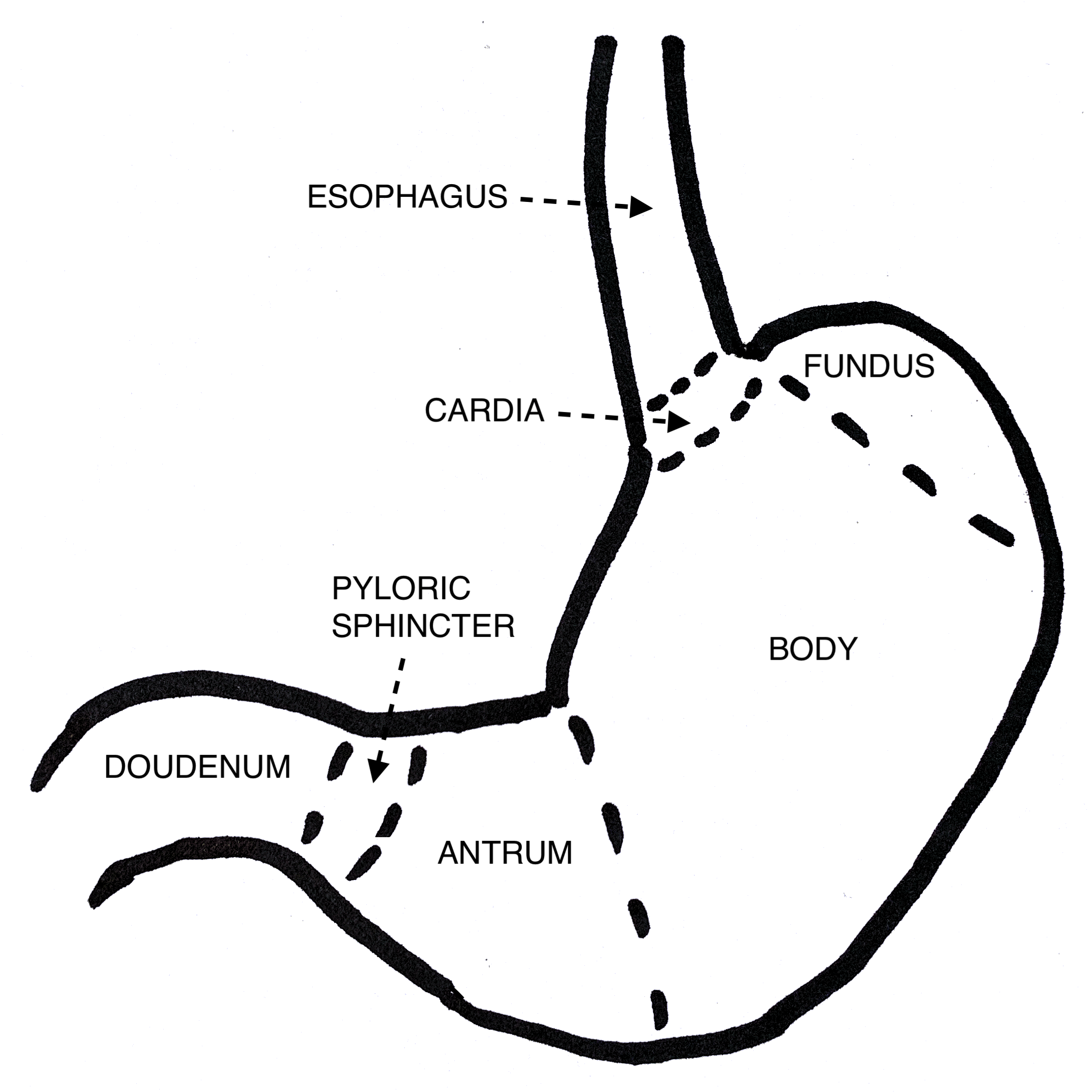
Mastery of gastric ultrasound requires knowledge of the anatomy of the stomach and nearby organs. The stomach is a “J”-shaped organ divided into four named regions: the cardia, fundus, body, and pylorus. The cardia is the region immediately distal to the esophagus. The fundus is the most cephalad portion of the stomach, lying above the cardiac notch. The body is the largest part of the stomach, providing space for food to mix with digestive enzymes. The funnel-shaped pylorus is the distal-most portion of the stomach, consisting of the antrum and the pyloric sphincter. The antrum lies between the gastric body and the pyloric sphincter, storing food before release through the pyloric sphincter into the duodenum. The antrum is the most important anatomical structure to visualize when performing gastric ultrasound.[12]
The stomach wall consists of three layers of alternating echogenicity, which can frequently be distinguished on ultrasound. The outermost layer is the serosa, which appears as a thin hyperechoic line. The muscularis propria, immediately deep to the serosa, appears as a thick, hypoechoic line and is easy to see on an ultrasound. The mucosa is the innermost layer of the stomach, which appears as a thin hyperechoic line. Occasionally, five layers of alternating echogenicity can be appreciated. The two innermost are thought to be artifactual due to the interface between the mucosal layer and fluid in the gastric lumen.[13]
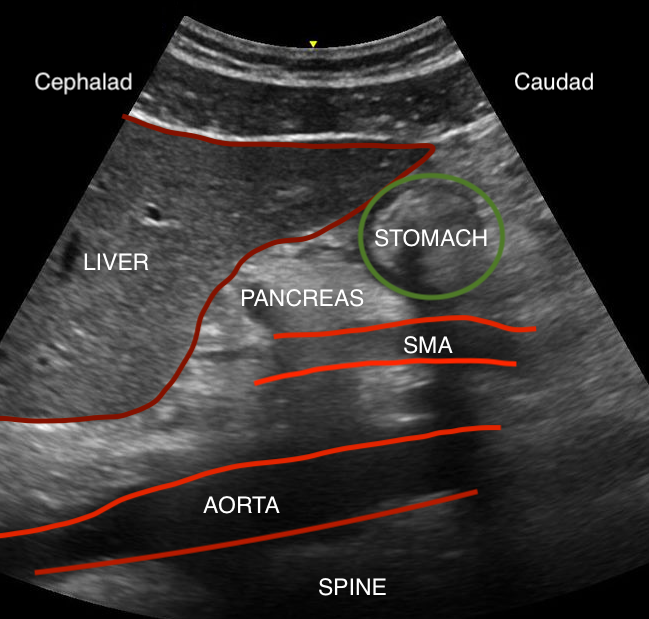
Gastric ultrasound is performed in the parasagittal imaging plane; thus, it is crucial to understand the relationship of adjacent organs to the stomach when viewed in this plane. The liver is easy to recognize due to its large size and highly vascular appearance. It should be located on the left of the screen (cephalad). The pancreas is located deep to the stomach and has a hyperechoic appearance. The bowel is difficult to visualize on ultrasound due to the presence of gas in the lumen but is generally located on the right side of the screen (caudad to the stomach).[14]
During the gastric ultrasound, several major blood vessels can be seen, including the aorta, the superior mesenteric artery (SMA), and the inferior vena cava (IVC). All appear anechoic (black) because they are filled with blood. The pulsatile SMA is the most superficial, located deep to the stomach but superficial to the aorta. The aorta and IVC can be challenging to distinguish, as both are large and located at similar depths. Only one should be visible in the parasagittal plane at a time because they run parallel to each other. The aorta has a thick wall, is pulsatile, and usually has a smaller diameter than the IVC. The IVC has a thin wall, if often compressible, and the diameter changes with the respiratory cycle, decreasing with inspiration and increasing during expiration. The aorta is seen anterior to the vertebral bodies and left of midline, while the IVC is at a similar depth but to the right of the midline.[5]
Indications
Gastric ultrasound provides a qualitative and quantitative assessment of gastric contents. Gastric ultrasound is most useful when fasting status is uncertain (e.g., unreliable historian, cognitive dysfunction, language barriers) or in physiologic states associated with delayed gastric emptying (e.g., diabetes mellitus, acute or chronic opioid use, pregnancy, abdominal infection).[15]
Information obtained from gastric ultrasound is used by anesthesia providers to determine if elective surgical cases should be postponed and to select the optimal induction and airway management technique for urgent or emergent procedures.[16]
Contraindications
There are no absolute contraindications to gastric ultrasound.
Gastric ultrasound is relatively contraindicated in patients with abdominal wounds, epigastric bandages, and those who cannot be safely positioned in the right lateral decubitus position (RLD).
Equipment
Virtually any diagnostic ultrasound machine can be used to perform a gastric ultrasound. Ideally, the machine should have the ability to measure the cross-sectional area (CSA). Abdominal imaging settings should be selected, if available. An appropriate imaging depth should be chosen to allow visualization of the abdominal aorta.
A low frequency (2 to 5 MHz) curved array probe is suitable for most patients. A higher frequency (5 to 13 MHz) linear probe may be suitable in small children, though care should be taken to ensure penetration is sufficient to allow imaging of the abdominal aorta.
Personnel
Gastric ultrasound can be performed and interpreted by a single, qualified clinician. However, additional help may be required to properly position small children or patients who are uncooperative, immobile, or sedated.
Preparation
The purpose of the exam should be explained to the patient prior to beginning. Expose the epigastrium, taking care to keep the patient’s chest and pelvic region covered. Clean towels should be used to protect the patient’s gown, clothing, and sheets from becoming soiled by gel. Position the ultrasound machine such that the screen is viewable while the exam is performed. Ideally, the examiner should be standing at the patient’s right side with the ultrasound machine positioned opposite the examiner on the patient’s left side.
Technique or Treatment
All imaging is performed in the parasagittal plane. Hold the transducer so that the orientation marker points towards the head (cephalad). If necessary, adjust the screen so that the orientation marker and cephalad structures are displayed on the left. The liver is easy to recognize cephalad structure, which should be on the left of the screen.
With the patient in the supine position, expose the epigastrium. Position the cephalad tip of the probe immediately below the xiphoid process. Confirm correct probe orientation after identifying the liver on the screen. Locate the great vessels (inferior vena cava or abdominal aorta) and adjust the image depth so that the posterior vessel border or vertebral bodies are visible at the bottom of the screen. Required depth varies significantly depending on the patient body habitus.
Scan the abdomen by sweeping the probe laterally, from left to right, keeping the probe perpendicular to the skin. Identify the stomach, liver, pancreas, superior mesenteric artery, aorta, and inferior vena cava. Examine and stomach and observe the characteristics of any stomach contents, noting the presence of solids, thick liquids, or clear fluids.[5]
- Note that the supine gastric exam is qualitative only and must be accompanied by examining the RLD position. A full stomach (presence of solids or thick liquids) can be confirmed in the supine position, but it cannot be ruled out. Moreover, gastric volume assessments cannot be accurately performed while supine.
After completing the exam in the supine position, place the patient in the right RLD position. This position facilitates the gravitational flow of stomach contents to the antrum, which increases the sensitivity of gastric ultrasound and facilitates gastric volume measurement.
With the patient in the RLD position, scan the abdomen, identifying the anatomic structures previously discussed. Occasionally, image depth must be increased to obtain adequate views of the great vessels of the abdomen.
Examine the contents of the stomach, again noting thick liquids or solids.[17][18]
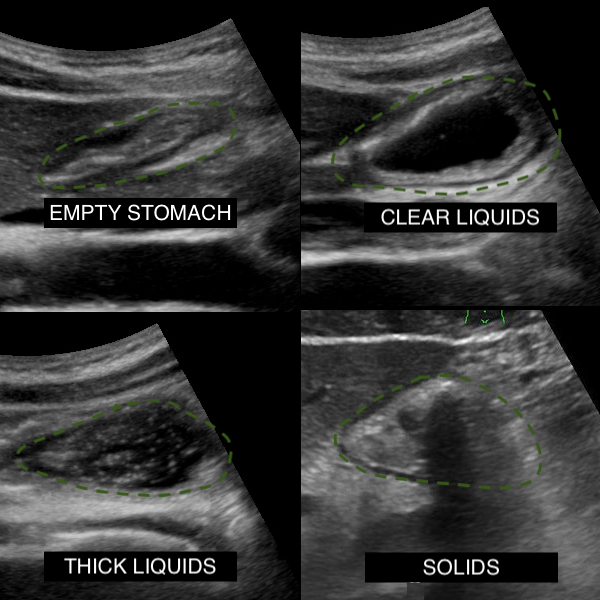
- Solids: Solids have a heterogeneous, “frosted glass” appearance on ultrasound. Structures located beyond solid food (e.g., aorta) may not be visible due to poor penetration of ultrasound waves beyond solid food.
- Thick liquids: Thick liquids (example: yogurt) appear hyperechoic and homogenous on gastric ultrasound.
- Clear liquids: Clear fluids appear hypoechoic (black) and homogenous. If the fluid was recently ingested, air bubbles (hyperechoic) might be present in the fluid, presenting a “starry night” appearance. The presence of clear liquids in the stomach should be followed by measuring antral CSA in the right lateral decubitus position, followed by calculating the estimated gastric volume (step 9).
- Empty: The empty stomach has a “bulls-eye” appearance, with a small or collapsed antrum surrounded by the sonographically distinct layers of the stomach wall. There is often a small volume of clear liquid (baseline gastric secretions) within a physiologically empty stomach.[2][10]
If the stomach contains only clear liquids, the volume can be estimated by measuring the CSA of the antrum at the level of the aorta. Care is necessary to ensure that measurements are taken at the aorta level rather than the IVC. Due to the funnel shape of the antrum, measurements at the level of the IVC will underestimate gastric volume, leading to false negatives.[19]
Calculate the estimated gastric volume: The volume of stomach contents (in milliliters) can be estimated by the following equation: 27 + (14.6 * CSA) – (1.28 * age).[20] For example, a 20-year-old, 80-kilogram (kg) patient with a CSA of 20 cm2 would have an estimated gastric volume of 27 + 14.6 * 20 – 1.28 * 20 = 293 milliliters (ml).
Gastric volumes <1.5 ml/kg are considered normal (consistent with baseline secretions), associated with a low risk of aspiration under anesthesia.[20] Volumes greater than 1.5 ml/kg are treated as positive findings. For the example patient above, the volume of gastric contents is 293/80 = 3.7 ml/kg, signifying a full stomach.
Clinical Significance
In the perioperative arena, the clinical significance of gastric ultrasound depends on the urgency of surgery. For elective procedures, cases should be canceled or postponed if the stomach contains solids, thick liquids, or a volume of clear fluids exceeding 1.5 ml/kg.[20]
In emergency procedures or those in which gastric emptying is unpredictable or may not improve with time (e.g., gastroparesis), the risk of aspiration and optimal timing of the case should be discussed with the patient and proceduralist. The anesthetic plan should include full aspiration precautions if the case must proceed. The patient should receive no sedation to preserve airway protective reflexes, or if sedation must be used, the airway should be protected with a rapid sequence induction and endotracheal intubation. Depending on the circumstances, the stomach should be decompressed with a nasogastric or oral gastric tube either before induction of anesthesia or following intubation.[10]
Enhancing Healthcare Team Outcomes
Gastric ultrasound is a useful diagnostic exam because it can reduce the risk of pulmonary aspiration of gastric contents. However, risk reduction requires effective communication and collaboration between all clinical members of each patient's care team. Surgical schedulers must ensure that patients receive instructions regarding appropriate fasting before surgery. On the day of a procedure, preoperative nurses should assess fasting status during the preoperative interview.
For surgical inpatients, the responsible provider (nurse practitioner, physician assistant, or physician) should ensure appropriate diet orders are placed the evening before a scheduled surgery. The anesthesiologist or nurse anesthetist is ultimately responsible for performing the final assessment and determining the most appropriate method for reducing the risk of aspiration. However, gastric ultrasound can be performed and interpreted by any qualified clinician.