Introduction
The adductor group of thigh muscles occupies the medial myofascial compartment of the thigh. This group of muscles generally originates from the pelvis and inserts on the femur. An exception, however, is the gracilis, which attaches to the proximal medial tibia as part of the pes anserine group rather than the femur.
The medial compartment muscles include the following:
- Pectineus
- Adductor longus
- Adductor brevis
- Gracilis
- Adductor magnus (the largest muscle in the group)
These muscles adduct the thigh and stabilize the pelvis, maintaining its balance during walking.
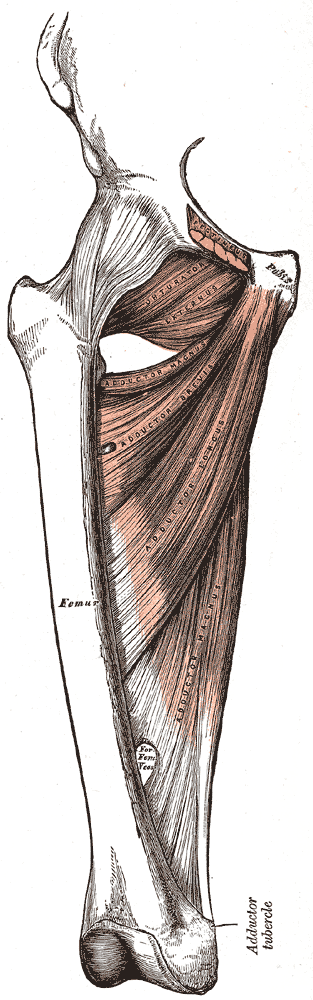
The adductor magnus is the largest and most posterior of the medial thigh compartment muscles (see Image. Medial Compartment of the Thigh). Some consider it the most powerful and most complex of the adductor group. It divides into its adductor (pubofemoral) and hamstring (ischiocondylar) portions. This article will focus on the adductor magnus.[1]
Structure and Function
The adductor magnus is a large triangular muscle with proximal tendinous attachments at the pubic bone's inferior ramus, ischial ramus, and ischial tuberosity. The adductor portion is attached proximally to the pubis' inferior ramus and ischial ramus. Its hamstring portion is attached proximally to the ischial tuberosity. Each portion of the adductor magnus muscle has distinct distal attachment points.
The adductor portion of the adductor magnus can be divided into two parts:
- Superior segment: originates from the pubic ramus. It is smaller and more horizontal. It inserts on the medial side of the gluteal tuberosity, medial to the gluteus maximus attachment. This portion of the muscle is in a plane that lies more anterior to the rest of the muscle and has also been termed the adductor minimus muscle by some authors.
- Inferior segment: arises from the ischial ramus. It is larger, extending laterally to insert on a broad aponeurosis on the linea aspera and the proximal portion of the femur's medial supracondylar line.
The inferior segment of the adductor portion contains 5 fibrous openings maintained by tendinous arches. The superior 4 openings, being small, allow the perforating branches and terminal portion of the profunda femoris artery to pass into the posterior compartment of the thigh. The larger 5th opening, known as the adductor hiatus, allows the passage of the femoral vessels from the adductor canal into the popliteal fossa.
The distal attachment of the adductor magnus' adductor portion on the linea aspera merges with the proximal attachment of the short head of the biceps femoris muscle. This merging allows the 2 muscles to work cooperatively to stabilize the femur and pelvis. The adductor portion of the adductor magnus is innervated by the posterior division of the obturator nerve (L2-L4).
The adductor magnus' hamstring portion is so named due to its similarity in structure, proximal attachment, and innervation to the hamstring muscles. This segment is nearly vertical in orientation. It runs from the ischial tuberosity to the adductor tubercle on the medial femoral condyle, passing through fibrous attachments to the femur's supracondylar line. The adductor magnus' hamstring segment is innervated by the tibial portion of the sciatic nerve (L4).
Both adductor and hamstring portions of the adductor magnus are thigh adductors, working synergistically during the gait cycle and controlling the pelvis for posture. The adductor portion also flexes the thigh. The hamstring portion also also extends the thigh.[2]
The adductor segment comprises approximately 70% of the adductor magnus muscle. Surface EMG studies of this large muscle segment are rare because of its depth. Most adductor magnus studies focus on the hamstring portion, which is accessible for surface EMG analysis. Whether or not the adductor magnus muscle affects postural control of the pelvis and lower extremities during the gait cycle is largely undetermined.
Embryology
The embryologic development of the adductor group first becomes evident in the proximal region of an 11-mm embryo. The mesenchyme in this area segregates into independent masses that will later turn into the different thigh muscles, including the adductor portion of the adductor magnus. When the embryo reaches 14 mm in length, the different muscles become evident, but their tendons are not yet prominent. Meanwhile, the hamstring portion of the adductor magnus differentiates from the dorsal thigh muscle blastema close to where the semimembranosus muscle develops.
As the embryo grows to 20 mm, the adductor and posterior thigh compartment muscles, along with their tendinous skeletal attachments, become distinct. The adductor and hamstring portions of the adductor magnus fuse at this point. Innervation to both segments develops from the anterior division of the lumbosacral plexus, suggesting that they develop from a primitive flexor origin.
Blood Supply and Lymphatics
The obturator artery supplies most of the medial thigh compartment. It branches out from the internal iliac artery, exiting the pelvis through the obturator foramen before entering the muscle compartment.
The adductor magnus' blood supply (see Image. Arterial Supply of the Lower Extremity) comes from several sources, namely:[3]
- Perforating branches of the profunda femoris artery: the primary blood supply of the muscle
- Medial femoral circumflex artery: supplies the superior portion of the muscle
- Femoral, popliteal, and genicular arteries: supply the inferior portion of the muscle
Lymphatic vessels from the adductor compartment muscles, including the adductor magnus, drain into the deep inguinal lymph nodes. These nodes are located in the medial segment of the femoral sheath and femoral triangle.
Nerves
In the embryo, adductor magnus innervation originates from the anterior lumbosacral plexus, obturator nerve, posterior L2-L4 nerve roots, and the tibial portion of the sciatic nerve (L4). The obturator nerve, which arises from the L2 to L4 nerve roots of the lumbar plexus, innervates most muscles in the adductor compartment.
Physiologic Variants
In 2011, Tubbs RS et al reported that more than half of the 20 adult cadavers and all 5 dissected fetuses in their study had an adductor minimus distinct from the adductor magnus muscle. Five others had the adductor minimus partially fused to the adductor magnus. The study also revealed that when the adductor minimus was absent or underdeveloped, the quadratus femoris extended inferiorly but stayed separated from the adductor magnus by a fascial layer.[4]
In an earlier study, Tubbs et al also noted that a vastoadductor membrane, a part of the intermuscular septum, can exist between the vastus medialis and adductor magnus. This membrane may compress the femoral artery before the latter passes through the adductor canal.[5]
Meanwhile, Takizawa et al challenged the long-held belief that the adductor portion of the adductor magnus is supplied by the posterior division of the obturator nerve, while the tibial portion of the sciatic nerve supplies the hamstring segment. In their study of 10 cadavers, they discovered that the adductor segment of the adductor magnus was innervated by both the posterior division of the obturator nerve and the tibial portion of the sciatic nerve. Another study by the same group revealed that over 90% of the distal adductor segment of the adductor magnus had dual innervation, particularly the posterior division of the obturator nerve and the tibial portion of the sciatic nerve.[4][6]
Additionally, Takizawa et al noted that the most proximal portion of the muscle had a different fiber morphology than the rest, so it is more suitable for stabilizing the lower limb. In contrast, the longer distal fibers are more functionally related to the semitendinosus, making them more able to extend the thigh's range of motion.[4]
Surgical Considerations
Obey et al [7] studied the proximal attachments of the hamstrings and adductor magnus on the ischial tuberosity in cadaveric specimens.[7] Hamstring tendon avulsion from the ischial tuberosity is increasingly recognized as an athletic injury that does not respond well to conservative treatment, has a poor outcome, and needs prompt surgical repair. An intact adductor magnus may mask a complete hamstring tendon avulsion on MRI, where it may resemble an intact but attenuated semimembranosus tendon.
The authors state that an intact adductor magnus may result in a misdiagnosis of a partial tear rather than a complete avulsion injury. They conclude that the adductor magnus is located medial to the hamstring origin on the ischial tuberosity. In some specimens, it looks like a sizable structure that may cause MRI interpretation errors in this area.[3]
Understanding the anatomical relationships between the adductor magnus and the hamstring tendons is crucial for appropriate diagnosis and management. The surgeon can perform the correct techniques, knowing the hamstring segment originates from the ischial tuberosity. As indicated in a study by Broski et al., radiologists also need to be aware of the attachment of the adductor magnus tendon on the ischial tuberosity when visualizing the area on MRI.[8]
Clinical Significance
Arnold and Delp studied the contribution of the medial hamstrings and adductor muscles in the crouched, internally rotated gait of individuals with cerebral palsy. Their findings were as follows:[9]
- The medial hamstrings, adductor brevis, adductor longus, and hamstring portion of the adductor magnus muscles had a slight internal rotation moment arm in the upright standing and normal femoral anteversion positions.
- The proximal adductor magnus and gracilis had a minor medial rotation moment arm.
- The middle and distal segments of the adductor segment of the adductor magnus had a negligible rotational moment arm.
However, the study found that the moment arms of these muscles changed with hip anteversion greater than 20° or knee flexion greater than 30°, with most becoming more externally biased. This finding is relevant when determining gait improvement strategies for these individuals. Caution must be exercised when treating muscles around the hip, as positional differences can influence muscular function.[10]
Other Issues
The adductor magnus muscle is both a dynamic stabilizer of the pelvis and femur and a prime femoral adductor. A portion of the muscle flexes and medially rotates the thigh. Another extends and laterally rotates the thigh. Both segments adduct the thigh. These actions make the adductor magnus similar in function to the deltoid.
The curvilinear pelvic attachment of the adductor magnus is also reminiscent of the curvilinear attachment of the deltoid on the spine of the scapula, acromion, and clavicle. Additionally, both the adductor magnus and deltoid serve as dynamic stabilizers of the ball and socket joints with which they are associated. These comparisons may aid students in correlating the upper and lower limb functions.