Continuing Education Activity
Arthrocentesis is a procedure performed to aspirate synovial fluid from a joint cavity. It has both diagnostic and therapeutic utilization. While arthrocentesis is deemed to be a minor surgical procedure, there is always potential to injure blood vessels, nerves, and tendons. Thus, the procedure should only be performed by clinicians with knowledge of the anatomy of the joint. This activity describes the indications, contraindications, complications, and technique involved in performing knee arthrocentesis and highlights the role of the interprofessional team in the management of patients undergoing this procedure.
Objectives:
- Identify the technique involved in performing knee arthrocentesis.
- Review the indications for knee arthrocentesis.
- Summarize the complications of knee arthrocentesis.
- Explain the importance of enhancing care coordination among interprofessional team members to ensure the correct and safe performance of arthrocentesis and thereby improve patient outcomes.
Introduction
Arthrocentesis is a procedure performed to aspirate synovial fluid from a joint cavity. It has both diagnostic and therapeutic uses. While arthrocentesis is deemed to be a minor surgical procedure, there is always the potential to injure blood vessels, nerves, and tendons. Thus, the procedure should only be performed by clinicians with extensive knowledge of the anatomy of joints. To minimize the risk of injury, the joint's extensor surface should be in extension with minimal flexion.[1][2]
Anatomy and Physiology
Anatomical considerations include:
- Surgeons can access the knee medially or laterally to the patella, superior or inferior to the patella.
- The patient should extend their knee with the quadriceps muscle relaxed at 20 degrees flexion.
- The physician should place their thumb on the patella and push it aside as they insert the needle.
- During the suprapatellar approach, they should place it 1 cm lateral and 1 cm superior.
- Upon identifying the midpoint of the patella, they should insert a needle either 1 cm lateral or medial.
- They should aim the needle posterior to the patella and up toward the joint space, then squeeze or "milk" both sides of the joint space to facilitate aspiration.
Indications
Therapeutic: Large and painful joint effusions can be aspirated for pain relief. Also, it can be used for intra-articular injection of certain medications (primarily steroids). Evaluate response to treatment.[2][3][4]
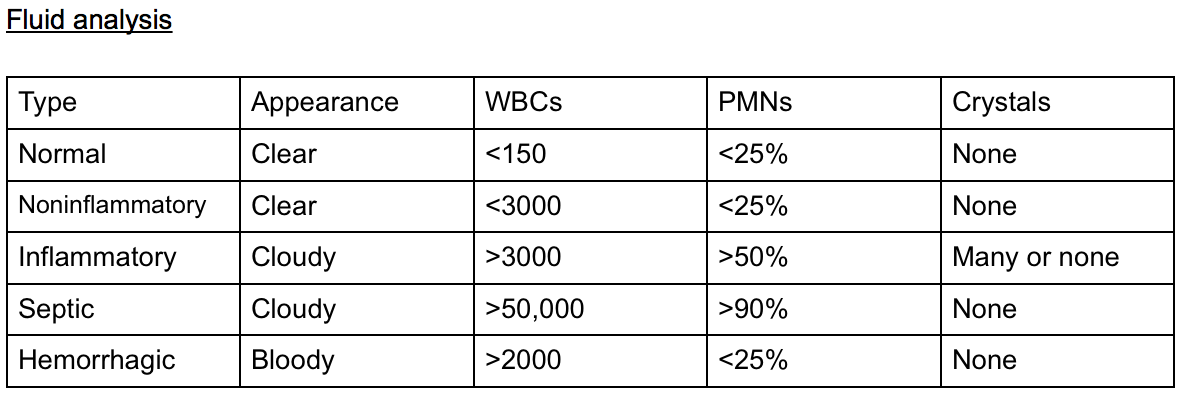
Diagnostic: Synovial fluid analysis can provide physicians with an unequivocal etiology of acute arthritis, specifically to differentiate between septic arthritis and an inflammatory cause of bloody mono-arthritis.
The procedure can be done in the clinic or the minor operating room.
Contraindications
No absolute contraindications. Relative contraindications include overlying cellulitis (potential intra-articular seeding of bacteria), coagulopathy/bleeding disorders, a joint prosthesis (preferably performed by orthopedic surgery in theatre ), acute fracture, adjacent osteomyelitis, and uncooperative patient.
Equipment
Skin cleansing solution (betadine, chlorhexidine, etc.), skin marking pen, sterile gloves, sterile gauze, 1% lidocaine, 10 cc syringe, 30 cc to 60 cc syringe, 18 g and 27 g needle, specimen tubes (cell count, gram stain, culture and sensitivity in addition to crystal analysis for gout and pseudogout).
Personnel
A skilled clinician can usually perform the procedure without an assistant. If the patient is anxious or exceptional circumstances apply, an assistant will make it much easier to perform the procedure.
Preparation
Anxious patients in pain or unable to cooperate with the procedure might require assistance and procedural sedation. It is a strong recommendation to utilize some type of local anesthesia. For most surgeons, lidocaine 1% will work to numb the skin. It is important to avoid deep injections with the local anesthetic because there is a risk that it may alter the synovial fluid analysis.
Technique or Treatment
The clinician or medical care professional must obtain informed consent. A timeout should take place to confirm the patient and correct joint. The most crucial step is having the patient lay in a comfortable position with the affected knee fully extended or flexed at 15 to 20 degrees with a towel roll under the knee. This position helps to facilitate procedure success by ensuring quadriceps muscle relaxation. The clinician should then locate the patella. The clinician may mark it with a marking pen.
The knee is the largest synovial cavity in the body and is easily accessible from either the medial or lateral aspect, and superior, inferior at the midpoint of the patella.
Sterilize area and drape in a typical sterile fashion.
Choose the approach, then use a small syringe and small-bore needle, draw up lidocaine and anesthetize superficial skin and then deeper tissue in the projected trajectory of joint aspiration to anesthetize the track.
- For the midpoint approach, insert an 18 g needle with 30 cc to 60 cc syringe one cm lateral or medial to the patella, directing the needle posterior and horizontal toward the intercondylar notch of the femur.
- Make sure to pull back on the syringe while inserting and stop once you aspirate synovial fluid.
- Attempt to aspirate as much fluid as possible.
- The superior approach is performed one cm superior and one cm medial or lateral to the patella, directing towards the femur's intercondylar notch.
- The infrapatellar approach requires the patient to be sitting upright, with the knee flexed at 90 degrees. Needle insertion is five mm below the patella's inferior border while also directing posterior to the patellar tendon, making this a less desirable approach.
“Milking” or compressing the joint can help facilitate the aspiration of fluid.
Transfer fluid to specimen tubes. Remove the needle from the joint and place bandage over the insertion site.
Complications
Local trauma, including damage to nearby structures, pain, infection, and reaccumulation of effusion.[5][6]
If the needle placement is poor or the synovium is thickened, it may result in a dry tap.
Hemarthrosis can occur if a large needle damages a blood vessel when performing multiple attempts. In most cases, the hemarthrosis presents within a few hours after the procedure. It is often associated with pain, stiffness, and swelling of the joint. The majority of hemarthrosis is self-limited and resolves within a few weeks. If the patient has a coagulopathy, it may need to be corrected, and consultation with a hematologist may help.
If arthrocentesis is performed through an infected area of skin to look for a septic joint, the patient must receive antibiotics promptly. If the fluid is frankly purulent, admission is recommended.
Clinical Significance
Arthrocentesis is performed to identify the etiology or pain relief, injection of medications, or effusion drainage. To avoid complications, the clinician should be familiar with the anatomy. The risk of complications can be minimized by using an appropriate technique.
Crystal analysis is usually an important result of a successful knee aspiration. The clinician commonly differentiates gout (negatively birefringent urate crystals), pseudogout (weakly positive birefringent crystals), and an infectious process.[7]
Synovial fluid associated with septic or infectious joint effusion is as follows:
- Total white blood cell count higher than 25,000/microliter (approximately 75% sensitive, 75% specific)
- Total white blood cell count higher than 50,000/microliter (approximately 60% sensitive, approximately 90% specific)
- Total white blood count higher than 100,000/microliter (approximately 20% sensitive, approximately 99% specific)
- PMN cell proportion 0.9 or higher (approximately 75% specific, 80% sensitive)
- Lactic dehydrogenase (LDH) concentration higher than 250 U/L (approximately 100% sensitive, 50% specific)
- Synovial glucose or serum glucose concentration lower than 0.5 (approximately 50% sensitive, 85% specific)
- Protein concentration higher than 3 g/dL (approximately 50% sensitive, 50% specific).
Enhancing Healthcare Team Outcomes
Knee joint aspiration is often an outpatient procedure. However, in most cases, the primary care provider or nurse practitioner should always consult with the orthopedic surgeon on management because there are many causes of a swollen knee. To avoid complications, the knee should only be aspirated by clinicians familiar with the anatomy.