Definition/Introduction
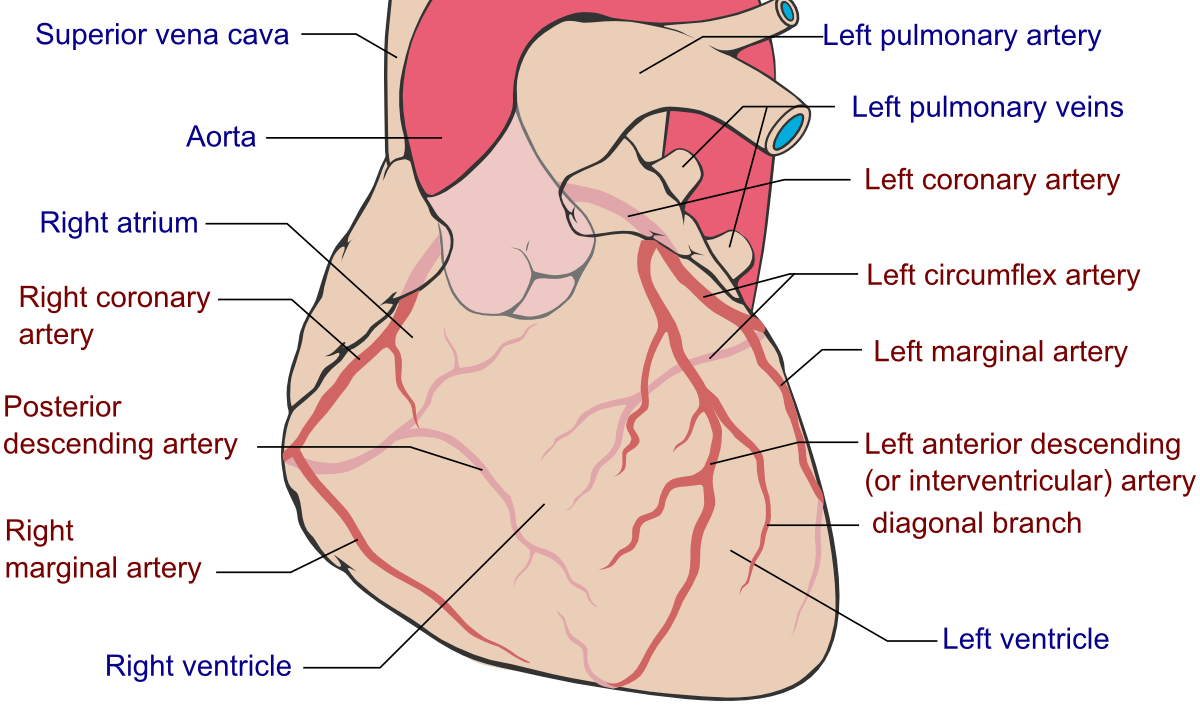
Heart dominance is described by which coronary artery branch gives off the posterior descending artery and supplies the inferior wall, and is characterized as left, right, or codominant. The posterior descending artery (PDA) is also known as the posterior interventricular artery because it runs along the posterior interventricular sulcus to the apex of the heart. It is at the apex where it meets the left anterior descending artery that is traveling along the anterior surface of the heart. The posterior descending artery is responsible for supplying the posterior third of the interventricular septum, including the posterior and inferior wall of the left ventricle. The vessel most commonly originates from either the right coronary artery (right dominant), left circumflex artery (left dominant), or both (codominant). There have been physiologic variants described in case reports such as an origin from the left anterior descending artery, referred to as “superdominant.”[1][2][3] Estimates are that 70 to 80% of the population is right heart dominant with the posterior descending artery originating from the right coronary artery. Approximately 5 to 10% of the population is left heart dominant with the PDA originating from the left circumflex artery, and about 10 to 20% is codominant with the PDA supplied by both the left circumflex artery and right coronary artery.[4] Small branches from the dominant artery perfuse the atrioventricular node.[5] Theoretically, decreased perfusion to the atrioventricular node may result in dysfunction, adding further significance to the cardiac dominance of the patient.