Introduction
Colon resection is the removal of part of or the entire colon, depending on the underlying etiology of the disease that necessitates the removal.[1][2]
Colon resection is the removal of part of or the entire colon, depending on the underlying etiology of the disease that necessitates the removal.[1][2]
The colon derives embryologically from the midgut and hindgut.
It is divided into the cecum, ascending, transverse, descending, and sigmoid colon and rectum.
Arteries, veins, and lymphatic drainage are located in the mesocolon, which during the oncological surgical resections of total mesorectal excision and complete mesocolic excision gets removed in its entirety corresponding to the part of the colon to be removed.
The commonest indication for surgical resection of the colon is a colorectal malignancy, and the resection should be carried out according to oncological principles:
Colonic resection is classified as major surgery and should not be undertaken if the patient is physically not fit to sustain a major procedure. Reversible and modifiable risk factors should be addressed before surgery, and postoperatively, a patient may require intensive or high dependency facilities.
Colonic resection can be carried out via open (laparotomy) or minimal access (laparoscopic, robotic) approaches.
Colonic resection requires a full contingent of operating theater personnel (scrub side, anesthesia side, and assistant to position the patient), an anesthetist, and a team of surgeons (at least one operating surgeon and one assistant).
Before surgery, the patient should be thoroughly evaluated.[3]
Bowel resection can be carried out as an open or laparoscopic procedure; the surgical principles remain the same.[4][5]
The key to adequate resection is the blood supply to the colon. Resection for benign disease does not need to be as extensive, but resection for malignancy should aim to resect the named colonic vessels supplying the cancer-bearing portion of the colon as close to their origin as possible to yield an adequate number of lymph nodes in the colonic mesentery (> 12).
The bowel proximal and distal to the resection have to be mobilized to allow a tension-free anastomosis, and the anastomosis should have a good blood supply. Depending on expertise and equipment available, a bowel anastomosis can be performed hand-sewn or stapled.
For example, a formal right hemicolectomy entails ligation of the ileocolic, right colic (if present), and right branch of the middle colic artery. Proximal bowel division is carried out at the terminal ileum, and distal bowel division at the transverse colon. The anastomosis is conventionally formed as a side-to-side between the terminal ileum and the transverse colon.
Resection of a sigmoid colon tumor entails ligation of the inferior mesenteric artery and inferior mesenteric vein. Proximal bowel division is carried out at the distal descending colon, and distal bowel division at the upper rectum, above the peritoneal reflection. The anastomosis is conventionally formed as an end-to-end between the descending colon and the upper rectum with the help of a circular stapling device inserted via the anal canal.
Procedure-related complications can be divided into complications encountered during the surgery and post-operative complications.[6][7][8]
Procedural complications include bleeding, most often venous in nature due to the handling of the mesocolon or during dissection of the greater omentum, and rarely from any of the named vessels.
However, an arterial bleed from the named vessels of the colon can be torrential and requires swift action, especially in laparoscopic procedures, where the bleeding can potentially obscure the view if it hits the camera.
Direct pressure where possible to temporarily arrest the bleeding buys time to strategize, reposition, request additional instruments, site further ports, if necessary, and definitively stop the bleed.
Another intra-operative complication is damage to surrounding structures. The structure most at risk is the left ureter. For left-sided surgery, it should always be identified. If an intra-operative injury (diathermy burn, transection) occurs and is recognized immediately, it can be repaired, and a ureteric stent should be placed to reduce the risk of stricture. If the injury is only diagnosed in the postoperative period, management depends on the extent and location of the injury, the general state of the patient, and the expertise available. A urological specialist should be consulted if available.
Post-operative complications include infections (wound, chest, urinary tract). Early mobilization, physiotherapy, incentive spirometry, and removal of urinary catheters can prevent infections. Wound infection risk in clean-contaminated surgery is greatly reduced by giving prophylactic antibiotics within one hour of skin incision.
Anastomotic leak is a dreaded complication for all surgeons performing colonic resection and primary anastomosis. A high index of suspicion is indicated if postoperatively, a patient does not progress as expected, as signs and symptoms can be subtle to start with, especially if the leak is in the pelvis and the patient has a defunctioning stoma. Patients may have pyrexia, tachycardia, cardiac arrhythmias (new-onset atrial fibrillation), complain of abdominal pain and bloating, and have a distended, tender, and potentially peritonitic abdomen. Inflammatory markers will be raised more markedly than expected in the postoperative period. Free air under the diaphragm may not be visible on an erect chest x-ray, but CT will show pneumoperitoneum and fluid around the anastomosis. In patients who have undergone anterior resection, it is advised to perform the scan with rectal contrast.
Depending on the severity of the leak and the patient's general state, the management can include all or parts of the following:
Prerequisites For Good Anastomosis
Adequate length of the colonic conduit for anterior resection:
While colon resection is done by the surgeon, the monitoring of the patient and preoperative workup is usually done by the anesthesiologist. Both before and after surgery, the nurse plays a vital role in bowel preparation and postoperative monitoring. The patient must have deep venous thrombosis prophylaxis and must be taught how to use the incentive spirometer. Physical therapy is usually consulted for ambulation of the patient in the post-operative period. [9][10]
Evidence-based Outcomes
Today elective colon resections have excellent outcomes. Most patients have a short stay in the hospital of about four days. By paying attention to detail, the risk of wound infection is also minimized. Current data indicate that laparoscopic colectomy is as effective as open colectomy in preventing recurrence of cancer. Further, several clinical trials have shown that the risk of seeding is not increased at the port sites.[11] [Level 2]
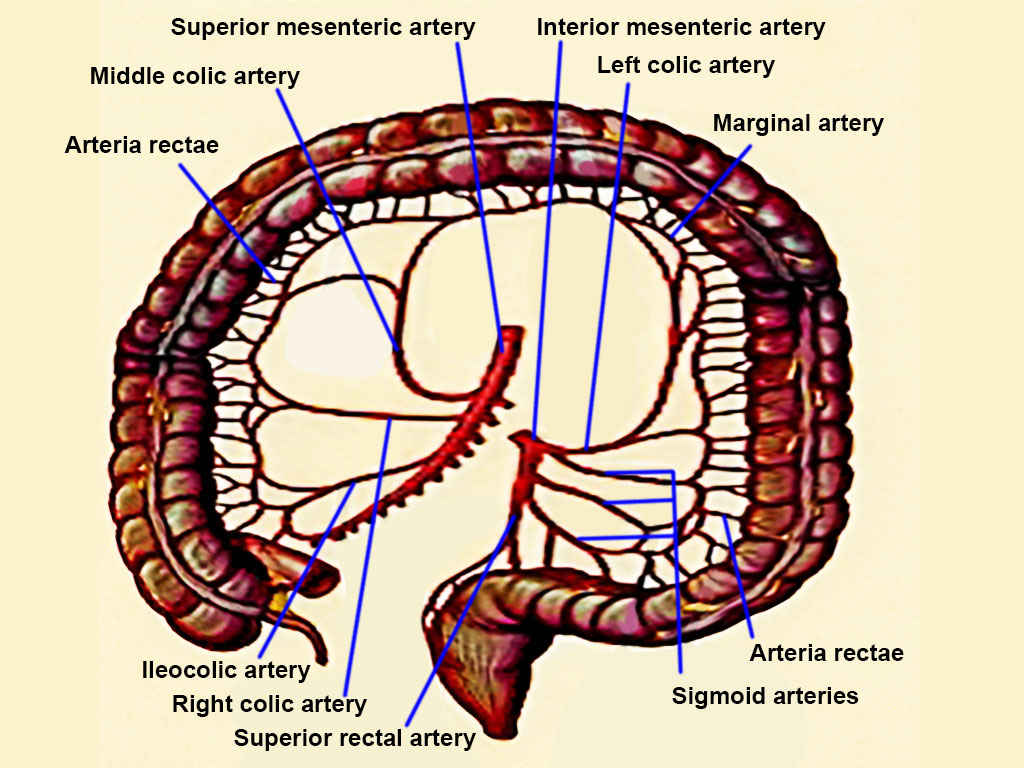
Arteries of the Large Intestine. The blood vessels shown in this image include the superior mesenteric, inferior mesenteric, left colic, marginal, arteria rectae, sigmoid, superior rectal, right colic, ileocolic, and middle colic arteries.
Contributed by T Silappathikaram
Hiroishi A, Yamada T, Morimoto T, Horikoshi K, Nakajima Y. Three-dimensional computed tomographic angiography with computed tomographic colonography for laparoscopic colorectal surgery. Japanese journal of radiology. 2018 Dec:36(12):698-705. doi: 10.1007/s11604-018-0775-7. Epub 2018 Sep 14 [PubMed PMID: 30218252]
Cleary RK, Morris AM, Chang GJ, Halverson AL. Controversies in Surgical Oncology: Does the Minimally Invasive Approach for Rectal Cancer Provide Equivalent Oncologic Outcomes Compared with the Open Approach? Annals of surgical oncology. 2018 Nov:25(12):3587-3595. doi: 10.1245/s10434-018-6740-y. Epub 2018 Sep 5 [PubMed PMID: 30187281]
Neale JA. Surgical Management of Diverticular Disease in the Elective Setting. Clinics in colon and rectal surgery. 2018 Jul:31(4):236-242. doi: 10.1055/s-0037-1607962. Epub 2018 Jun 22 [PubMed PMID: 29942214]
Zattoni D, Popeskou GS, Christoforidis D. Left colon resection with transrectal specimen extraction: current status. Techniques in coloproctology. 2018 Jun:22(6):411-423. doi: 10.1007/s10151-018-1806-1. Epub 2018 Jun 12 [PubMed PMID: 29948523]
Zhu XL, Yan PJ, Yao L, Liu R, Wu DW, Du BB, Yang KH, Guo TK, Yang XF. Comparison of Short-Term Outcomes Between Robotic-Assisted and Laparoscopic Surgery in Colorectal Cancer. Surgical innovation. 2019 Feb:26(1):57-65. doi: 10.1177/1553350618797822. Epub 2018 Sep 7 [PubMed PMID: 30191755]
Špičák J, Kučera M, Suchánková G. Diverticular disease: diagnosis and treatment. Vnitrni lekarstvi. 2018 Summer:64(6):621-634 [PubMed PMID: 30223660]
Alhassan N, Yang M, Wong-Chong N, Liberman AS, Charlebois P, Stein B, Fried GM, Lee L. Comparison between conventional colectomy and complete mesocolic excision for colon cancer: a systematic review and pooled analysis : A review of CME versus conventional colectomies. Surgical endoscopy. 2019 Jan:33(1):8-18. doi: 10.1007/s00464-018-6419-2. Epub 2018 Sep 12 [PubMed PMID: 30209606]
Level 1 (high-level) evidenceLasinski AM, Gil L, Kothari AN, Anstadt MJ, Gonzalez RP. Defining Outcomes after Colon Resection in Blunt Trauma: Is Diversion or Primary Anastomosis More Favorable? The American surgeon. 2018 Aug 1:84(8):1288-1293 [PubMed PMID: 30185302]
Trautmann F, Reißfelder C, Pecqueux M, Weitz J, Schmitt J. Evidence-based quality standards improve prognosis in colon cancer care. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2018 Sep:44(9):1324-1330. doi: 10.1016/j.ejso.2018.05.013. Epub 2018 May 17 [PubMed PMID: 29885983]
Level 2 (mid-level) evidenceExpert Panel on Gastrointestinal Imaging:, Fowler KJ, Kaur H, Cash BD, Feig BW, Gage KL, Garcia EM, Hara AK, Herman JM, Kim DH, Lambert DL, Levy AD, Peterson CM, Scheirey CD, Small W Jr, Smith MP, Lalani T, Carucci LR. ACR Appropriateness Criteria(®) Pretreatment Staging of Colorectal Cancer. Journal of the American College of Radiology : JACR. 2017 May:14(5S):S234-S244. doi: 10.1016/j.jacr.2017.02.012. Epub [PubMed PMID: 28473079]
McCombie AM, Frizelle F, Bagshaw PF, Frampton CM, Hewett PJ, McMurrick PJ, Rieger N, Solomon MJ, Stevenson AR, ALCCaS Trial group. The ALCCaS Trial: A Randomized Controlled Trial Comparing Quality of Life Following Laparoscopic Versus Open Colectomy for Colon Cancer. Diseases of the colon and rectum. 2018 Oct:61(10):1156-1162. doi: 10.1097/DCR.0000000000001165. Epub [PubMed PMID: 30192324]
Level 2 (mid-level) evidence