Introduction
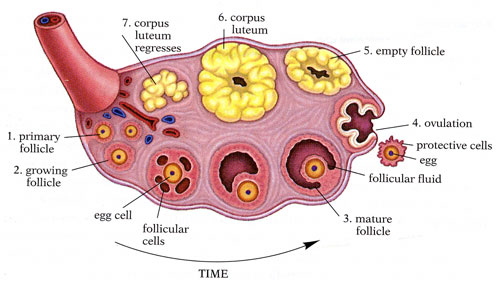
The corpus luteum is a vital yet temporary organ that plays a crucial role in fertility during the luteal phase. An endocrine structure in females exists within the ovary once the ovarian follicle releases a mature ovum during ovulation. See Image. Anatomy of the Internal Structures of the Ovary. The secretion of hormones from the corpus luteum stops within 14 days after ovulation if the oocyte is not fertilized. It then degenerates into a scar within the ovary, known as corpus albicans. The corpus luteum's role is to maintain a uterine environment that allows for implementation and pregnancy. This occurs by the release of pregnancy-related hormones and regulation of the hypothalamic-pituitary access through inhibition of gonadotropin-releasing hormone from the hypothalamus, which in turn decreases the luteinizing hormone (LH) and follicle-stimulating hormone (FSH) released from the anterior pituitary. The primary hormone produced by the corpus luteum is progesterone, but it also produces inhibin A and estradiol. In the absence of fertilization, the corpus luteum regresses over time. A corpus luteum develops each time a woman ovulates so that she produces a corpus luteum numerous times throughout her lifetime.