[1]
Irwin RS, French CL, Chang AB, Altman KW, CHEST Expert Cough Panel*. Classification of Cough as a Symptom in Adults and Management Algorithms: CHEST Guideline and Expert Panel Report. Chest. 2018 Jan:153(1):196-209. doi: 10.1016/j.chest.2017.10.016. Epub 2017 Nov 10
[PubMed PMID: 29080708]
[2]
Song WJ, Morice AH, Kim MH, Lee SE, Jo EJ, Lee SM, Han JW, Kim TH, Kim SH, Jang HC, Kim KW, Cho SH, Min KU, Chang YS. Cough in the elderly population: relationships with multiple comorbidity. PloS one. 2013:8(10):e78081. doi: 10.1371/journal.pone.0078081. Epub 2013 Oct 21
[PubMed PMID: 24205100]
[3]
Morice AH, McGarvey L, Pavord I, British Thoracic Society Cough Guideline Group. Recommendations for the management of cough in adults. Thorax. 2006 Sep:61 Suppl 1(Suppl 1):i1-24
[PubMed PMID: 16936230]
[4]
Ptak K, Cichocka-Jarosz E, Kwinta P. [Chronic cough in children]. Developmental period medicine. 2018:22(4):329-340
[PubMed PMID: 30636230]
[5]
Koehler U, Hildebrandt O, Walliczek-Dworschak U, Nikolaizik W, Weissflog A, Urban C, Kerzel S, Sohrabi K, Groß V. [Chronic cough - New diagnostic options for evaluation?]. Laryngo- rhino- otologie. 2019 Jan:98(1):14-20. doi: 10.1055/a-0790-0777. Epub 2019 Jan 8
[PubMed PMID: 30620964]
[6]
Morice AH, Millqvist E, Bieksiene K, Birring SS, Dicpinigaitis P, Domingo Ribas C, Hilton Boon M, Kantar A, Lai K, McGarvey L, Rigau D, Satia I, Smith J, Song WJ, Tonia T, van den Berg JWK, van Manen MJG, Zacharasiewicz A. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. The European respiratory journal. 2020 Jan:55(1):. doi: 10.1183/13993003.01136-2019. Epub 2020 Jan 2
[PubMed PMID: 31515408]
[7]
Hao H, Pan Y, Xu Z, Xu Z, Bao W, Xue Y, Lv C, Lin J, Zhang Y, Zhang M. Prediction of bronchodilation test in adults with chronic cough suspected of cough variant asthma. Frontiers in medicine. 2022:9():987887. doi: 10.3389/fmed.2022.987887. Epub 2022 Dec 9
[PubMed PMID: 36569143]
[9]
Diab N, Patel M, O'Byrne P, Satia I. Narrative Review of the Mechanisms and Treatment of Cough in Asthma, Cough Variant Asthma, and Non-asthmatic Eosinophilic Bronchitis. Lung. 2022 Dec:200(6):707-716. doi: 10.1007/s00408-022-00575-6. Epub 2022 Oct 13
[PubMed PMID: 36227349]
Level 3 (low-level) evidence
[10]
Lai K, Liu B, Xu D, Han L, Lin L, Xi Y, Wang F, Chen R, Luo W, Chen Q, Zhong N. Will nonasthmatic eosinophilic bronchitis develop into chronic airway obstruction?: a prospective, observational study. Chest. 2015 Oct:148(4):887-894. doi: 10.1378/chest.14-2351. Epub
[PubMed PMID: 25905627]
Level 2 (mid-level) evidence
[11]
Brightling CE, Symon FA, Birring SS, Bradding P, Wardlaw AJ, Pavord ID. Comparison of airway immunopathology of eosinophilic bronchitis and asthma. Thorax. 2003 Jun:58(6):528-32
[PubMed PMID: 12775868]
[12]
Park SW, Lee YM, Jang AS, Lee JH, Hwangbo Y, Kim DJ, Park CS. Development of chronic airway obstruction in patients with eosinophilic bronchitis: a prospective follow-up study. Chest. 2004 Jun:125(6):1998-2004
[PubMed PMID: 15189914]
[13]
Malesker MA, Callahan-Lyon P, Madison JM, Ireland B, Irwin RS, CHEST Expert Cough Panel. Chronic Cough Due to Stable Chronic Bronchitis: CHEST Expert Panel Report. Chest. 2020 Aug:158(2):705-718. doi: 10.1016/j.chest.2020.02.015. Epub 2020 Feb 24
[PubMed PMID: 32105719]
[14]
Irwin RS. Chronic cough due to gastroesophageal reflux disease: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan:129(1 Suppl):80S-94S. doi: 10.1378/chest.129.1_suppl.80S. Epub
[PubMed PMID: 16428697]
Level 1 (high-level) evidence
[15]
Wang S, Wen S, Bai X, Zhang M, Zhu Y, Wu M, Lu L, Shi C, Yu L, Xu X. Diagnostic value of reflux episodes in gastroesophageal reflux-induced chronic cough: a novel predictive indicator. Therapeutic advances in chronic disease. 2022:13():20406223221117455. doi: 10.1177/20406223221117455. Epub 2022 Aug 17
[PubMed PMID: 36003286]
Level 3 (low-level) evidence
[16]
Kahrilas PJ, Altman KW, Chang AB, Field SK, Harding SM, Lane AP, Lim K, McGarvey L, Smith J, Irwin RS, CHEST Expert Cough Panel. Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. Chest. 2016 Dec:150(6):1341-1360. doi: 10.1016/j.chest.2016.08.1458. Epub 2016 Sep 7
[PubMed PMID: 27614002]
[17]
Lucanska M, Hajtman A, Calkovsky V, Kunc P, Pecova R. Upper Airway Cough Syndrome in Pathogenesis of Chronic Cough. Physiological research. 2020 Mar 27:69(Suppl 1):S35-S42
[PubMed PMID: 32228010]
[18]
Woo KS, Nicholls MG. High prevalence of persistent cough with angiotensin converting enzyme inhibitors in Chinese. British journal of clinical pharmacology. 1995 Aug:40(2):141-4
[PubMed PMID: 8562296]
[19]
Berkin KE, Ball SG. Cough and angiotensin converting enzyme inhibition. British medical journal (Clinical research ed.). 1988 May 7:296(6632):1279
[PubMed PMID: 3133049]
[20]
Borghi C, Cicero AF, Agnoletti D, Fiorini G. Pathophysiology of cough with angiotensin-converting enzyme inhibitors: How to explain within-class differences? European journal of internal medicine. 2023 Apr:110():10-15. doi: 10.1016/j.ejim.2023.01.005. Epub 2023 Jan 8
[PubMed PMID: 36628825]
[21]
Samizo K, Kawabe E, Hinotsu S, Sato T, Kageyama S, Hamada C, Ohashi Y, Kubota K. Comparison of losartan with ACE inhibitors and dihydropyridine calcium channel antagonists: a pilot study of prescription-event monitoring in Japan. Drug safety. 2002:25(11):811-21
[PubMed PMID: 12222991]
Level 3 (low-level) evidence
[22]
Fahim A, Morice AH. Heightened cough sensitivity secondary to latanoprost. Chest. 2009 Nov:136(5):1406-1407. doi: 10.1378/chest.09-0070. Epub
[PubMed PMID: 19892680]
[23]
Rosen MJ. Chronic cough due to bronchiectasis: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan:129(1 Suppl):122S-131S. doi: 10.1378/chest.129.1_suppl.122S. Epub
[PubMed PMID: 16428701]
Level 1 (high-level) evidence
[24]
Polverino E, Dimakou K, Hurst J, Martinez-Garcia MA, Miravitlles M, Paggiaro P, Shteinberg M, Aliberti S, Chalmers JD. The overlap between bronchiectasis and chronic airway diseases: state of the art and future directions. The European respiratory journal. 2018 Sep:52(3):. pii: 1800328. doi: 10.1183/13993003.00328-2018. Epub 2018 Sep 15
[PubMed PMID: 30049739]
Level 3 (low-level) evidence
[25]
Poe RH, Harder RV, Israel RH, Kallay MC. Chronic persistent cough. Experience in diagnosis and outcome using an anatomic diagnostic protocol. Chest. 1989 Apr:95(4):723-8
[PubMed PMID: 2924600]
[26]
Davis SF, Sutter RW, Strebel PM, Orton C, Alexander V, Sanden GN, Cassell GH, Thacker WL, Cochi SL. Concurrent outbreaks of pertussis and Mycoplasma pneumoniae infection: clinical and epidemiological characteristics of illnesses manifested by cough. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1995 Mar:20(3):621-8
[PubMed PMID: 7756486]
Level 2 (mid-level) evidence
[27]
Yaari E, Yafe-Zimerman Y, Schwartz SB, Slater PE, Shvartzman P, Andoren N, Branski D, Kerem E. Clinical manifestations of Bordetella pertussis infection in immunized children and young adults. Chest. 1999 May:115(5):1254-8
[PubMed PMID: 10334136]
[28]
Song WJ, Hui CKM, Hull JH, Birring SS, McGarvey L, Mazzone SB, Chung KF. Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses. The Lancet. Respiratory medicine. 2021 May:9(5):533-544. doi: 10.1016/S2213-2600(21)00125-9. Epub 2021 Apr 12
[PubMed PMID: 33857435]
[29]
Chung KF, McGarvey L, Mazzone S. Chronic cough and cough hypersensitivity syndrome. The Lancet. Respiratory medicine. 2016 Dec:4(12):934-935. doi: 10.1016/S2213-2600(16)30373-3. Epub 2016 Nov 22
[PubMed PMID: 27890496]
[30]
Mazzone SB, Satia I, McGarvey L, Song WJ, Chung KF. Chronic cough and cough hypersensitivity: from mechanistic insights to novel antitussives. The Lancet. Respiratory medicine. 2022 Dec:10(12):1113-1115. doi: 10.1016/S2213-2600(22)00404-0. Epub 2022 Nov 10
[PubMed PMID: 36372083]
[31]
Chung KF, McGarvey L, Mazzone SB. Chronic cough as a neuropathic disorder. The Lancet. Respiratory medicine. 2013 Jul:1(5):414-22. doi: 10.1016/S2213-2600(13)70043-2. Epub 2013 May 3
[PubMed PMID: 24429206]
[32]
Iyer S, Roughley A, Rider A, Taylor-Stokes G. The symptom burden of non-small cell lung cancer in the USA: a real-world cross-sectional study. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer. 2014 Jan:22(1):181-7. doi: 10.1007/s00520-013-1959-4. Epub 2013 Sep 12
[PubMed PMID: 24026981]
Level 2 (mid-level) evidence
[33]
Molassiotis A, Smith JA, Mazzone P, Blackhall F, Irwin RS, CHEST Expert Cough Panel. Symptomatic Treatment of Cough Among Adult Patients With Lung Cancer: CHEST Guideline and Expert Panel Report. Chest. 2017 Apr:151(4):861-874. doi: 10.1016/j.chest.2016.12.028. Epub 2017 Jan 17
[PubMed PMID: 28108179]
[34]
Bargagli E, Di Masi M, Perruzza M, Vietri L, Bergantini L, Torricelli E, Biadene G, Fontana G, Lavorini F. The pathogenetic mechanisms of cough in idiopathic pulmonary fibrosis. Internal and emergency medicine. 2019 Jan:14(1):39-43. doi: 10.1007/s11739-018-1960-5. Epub 2018 Sep 29
[PubMed PMID: 30269188]
[35]
Key AL, Holt K, Hamilton A, Smith JA, Earis JE. Objective cough frequency in Idiopathic Pulmonary Fibrosis. Cough (London, England). 2010 Jun 21:6():4. doi: 10.1186/1745-9974-6-4. Epub 2010 Jun 21
[PubMed PMID: 20565979]
[36]
Birring SS, Kavanagh JE, Irwin RS, Keogh KA, Lim KG, Ryu JH, Collaborators. Treatment of Interstitial Lung Disease Associated Cough: CHEST Guideline and Expert Panel Report. Chest. 2018 Oct:154(4):904-917. doi: 10.1016/j.chest.2018.06.038. Epub 2018 Jul 20
[PubMed PMID: 30036496]
[37]
Tobin RW, Pope CE 2nd, Pellegrini CA, Emond MJ, Sillery J, Raghu G. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. American journal of respiratory and critical care medicine. 1998 Dec:158(6):1804-8
[PubMed PMID: 9847271]
[38]
Birring SS, Parker D, McKenna S, Hargadon B, Brightling CE, Pavord ID, Bradding P. Sputum eosinophilia in idiopathic pulmonary fibrosis. Inflammation research : official journal of the European Histamine Research Society ... [et al.]. 2005 Feb:54(2):51-6
[PubMed PMID: 15750711]
[39]
Birring SS, Brightling CE, Symon FA, Barlow SG, Wardlaw AJ, Pavord ID. Idiopathic chronic cough: association with organ specific autoimmune disease and bronchoalveolar lymphocytosis. Thorax. 2003 Dec:58(12):1066-70
[PubMed PMID: 14645977]
[40]
Chung KF, McGarvey L, Song WJ, Chang AB, Lai K, Canning BJ, Birring SS, Smith JA, Mazzone SB. Cough hypersensitivity and chronic cough. Nature reviews. Disease primers. 2022 Jun 30:8(1):45. doi: 10.1038/s41572-022-00370-w. Epub 2022 Jun 30
[PubMed PMID: 35773287]
[41]
Maio S, Baldacci S, Carrozzi L, Pistelli F, Simoni M, Angino A, La Grutta S, Muggeo V, Viegi G. 18-yr cumulative incidence of respiratory/allergic symptoms/diseases and risk factors in the Pisa epidemiological study. Respiratory medicine. 2019 Oct-Nov:158():33-41. doi: 10.1016/j.rmed.2019.09.013. Epub 2019 Sep 24
[PubMed PMID: 31585374]
Level 2 (mid-level) evidence
[42]
Barbee RA, Halonen M, Kaltenborn WT, Burrows B. A longitudinal study of respiratory symptoms in a community population sample. Correlations with smoking, allergen skin-test reactivity, and serum IgE. Chest. 1991 Jan:99(1):20-6
[PubMed PMID: 1984955]
[43]
Janson C, Anto J, Burney P, Chinn S, de Marco R, Heinrich J, Jarvis D, Kuenzli N, Leynaert B, Luczynska C, Neukirch F, Svanes C, Sunyer J, Wjst M, European Community Respiratory Health Survey II. The European Community Respiratory Health Survey: what are the main results so far? European Community Respiratory Health Survey II. The European respiratory journal. 2001 Sep:18(3):598-611
[PubMed PMID: 11589359]
Level 3 (low-level) evidence
[44]
Song WJ, Chang YS, Faruqi S, Kim JY, Kang MG, Kim S, Jo EJ, Kim MH, Plevkova J, Park HW, Cho SH, Morice AH. The global epidemiology of chronic cough in adults: a systematic review and meta-analysis. The European respiratory journal. 2015 May:45(5):1479-81. doi: 10.1183/09031936.00218714. Epub 2015 Feb 5
[PubMed PMID: 25657027]
Level 1 (high-level) evidence
[45]
Dicpinigaitis PV, Allusson VR, Baldanti A, Nalamati JR. Ethnic and gender differences in cough reflex sensitivity. Respiration; international review of thoracic diseases. 2001:68(5):480-2
[PubMed PMID: 11694809]
[46]
Kang MG, Song WJ, Kim HJ, Won HK, Sohn KH, Kang SY, Jo EJ, Kim MH, Kim SH, Kim SH, Park HW, Chang YS, Lee BJ, Morice AH, Cho SH. Point prevalence and epidemiological characteristics of chronic cough in the general adult population: The Korean National Health and Nutrition Examination Survey 2010-2012. Medicine. 2017 Mar:96(13):e6486. doi: 10.1097/MD.0000000000006486. Epub
[PubMed PMID: 28353590]
Level 2 (mid-level) evidence
[47]
Yang X, Chung KF, Huang K. Worldwide prevalence, risk factors and burden of chronic cough in the general population: a narrative review. Journal of thoracic disease. 2023 Apr 28:15(4):2300-2313. doi: 10.21037/jtd-22-1435. Epub 2023 Apr 26
[PubMed PMID: 37197554]
Level 3 (low-level) evidence
[48]
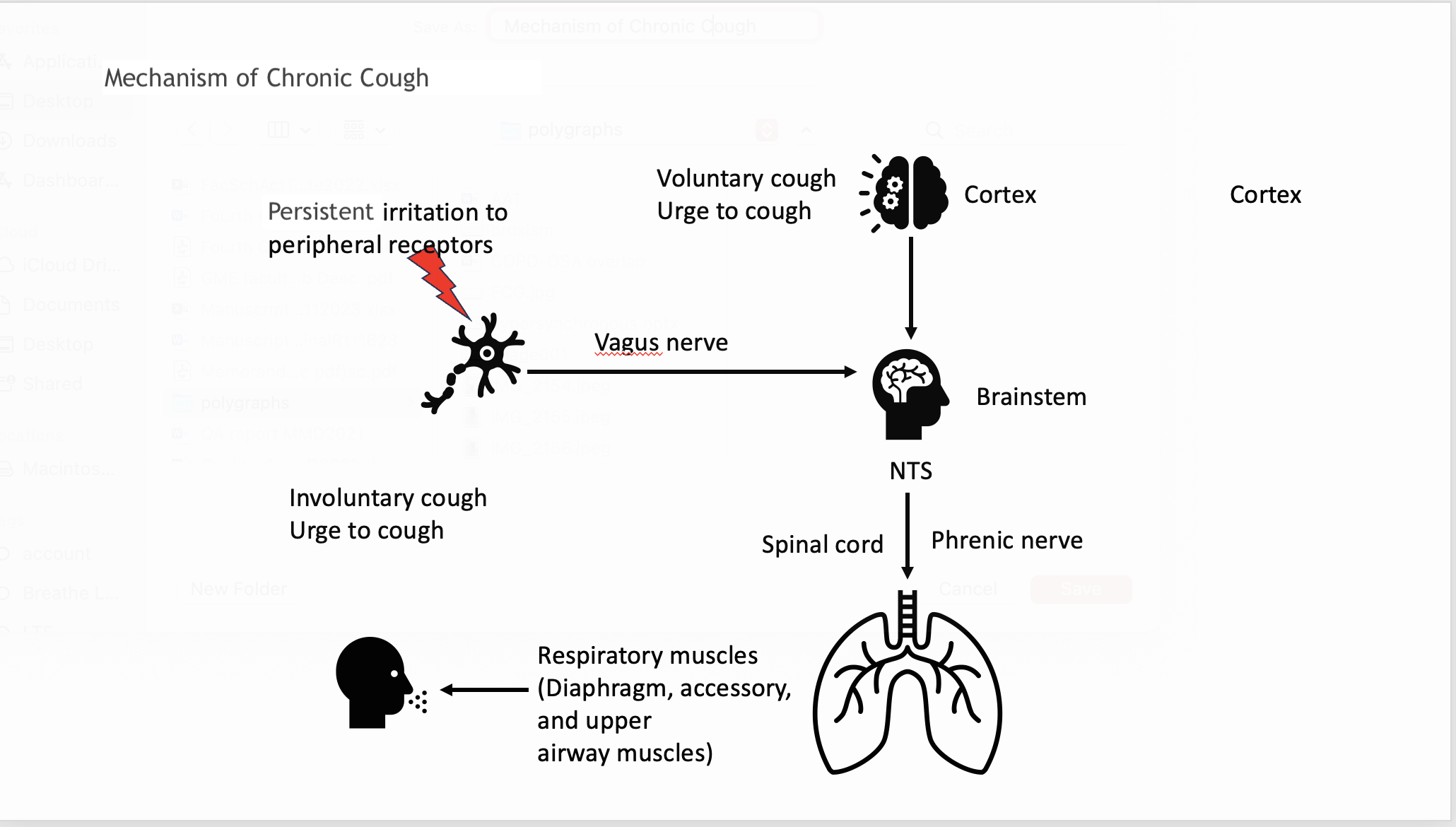
Narula M, McGovern AE, Yang SK, Farrell MJ, Mazzone SB. Afferent neural pathways mediating cough in animals and humans. Journal of thoracic disease. 2014 Oct:6(Suppl 7):S712-9. doi: 10.3978/j.issn.2072-1439.2014.03.15. Epub
[PubMed PMID: 25383205]
Level 3 (low-level) evidence
[49]
Canning BJ, Chang AB, Bolser DC, Smith JA, Mazzone SB, McGarvey L, CHEST Expert Cough Panel. Anatomy and neurophysiology of cough: CHEST Guideline and Expert Panel report. Chest. 2014 Dec:146(6):1633-1648. doi: 10.1378/chest.14-1481. Epub
[PubMed PMID: 25188530]
[50]
Fracchia MS, Diercks G, Cook A, Hersh C, Hardy S, Hartnick M, Hartnick C. The diagnostic role of triple endoscopy in pediatric patients with chronic cough. International journal of pediatric otorhinolaryngology. 2019 Jan:116():58-61. doi: 10.1016/j.ijporl.2018.10.017. Epub 2018 Oct 13
[PubMed PMID: 30554708]
[51]
Moore A, Harnden A, Grant CC, Patel S, Irwin RS, CHEST Expert Cough Panel. Clinically Diagnosing Pertussis-associated Cough in Adults and Children: CHEST Guideline and Expert Panel Report. Chest. 2019 Jan:155(1):147-154. doi: 10.1016/j.chest.2018.09.027. Epub 2018 Oct 12
[PubMed PMID: 30321509]
[52]
Gibson PG, Vertigan AE. Management of chronic refractory cough. BMJ (Clinical research ed.). 2015 Dec 14:351():h5590. doi: 10.1136/bmj.h5590. Epub 2015 Dec 14
[PubMed PMID: 26666537]
[53]
Bhalla K, Nehra D, Nanda S, Verma R, Gupta A, Mehra S. Prevalence of bronchial asthma and its associated risk factors in school-going adolescents in Tier-III North Indian City. Journal of family medicine and primary care. 2018 Nov-Dec:7(6):1452-1457. doi: 10.4103/jfmpc.jfmpc_117_18. Epub
[PubMed PMID: 30613541]
[54]
. "ERS guidelines on the diagnosis and treatment of chronic cough in adults and children." Alyn H. Morice, Eva Millqvist, Kristina Bieksiene, Surinder S. Birring, Peter Dicpinigaitis, Christian Domingo Ribas, Michele Hilton Boon, Ahmad Kantar, Kefang Lai, Lorcan McGarvey, David Rigau, Imran Satia, Jacky Smith, Woo-Jung Song, Thomy Tonia, Jan W.K. van den Berg, Mirjam J.G. van Manen and Angela Zacharasiewicz. Eur Respir J 2020; 55: 1901136. The European respiratory journal. 2020 Nov:56(5):. pii: 1951136. doi: 10.1183/13993003.51136-2019. Epub 2020 Nov 19
[PubMed PMID: 33214170]
[55]
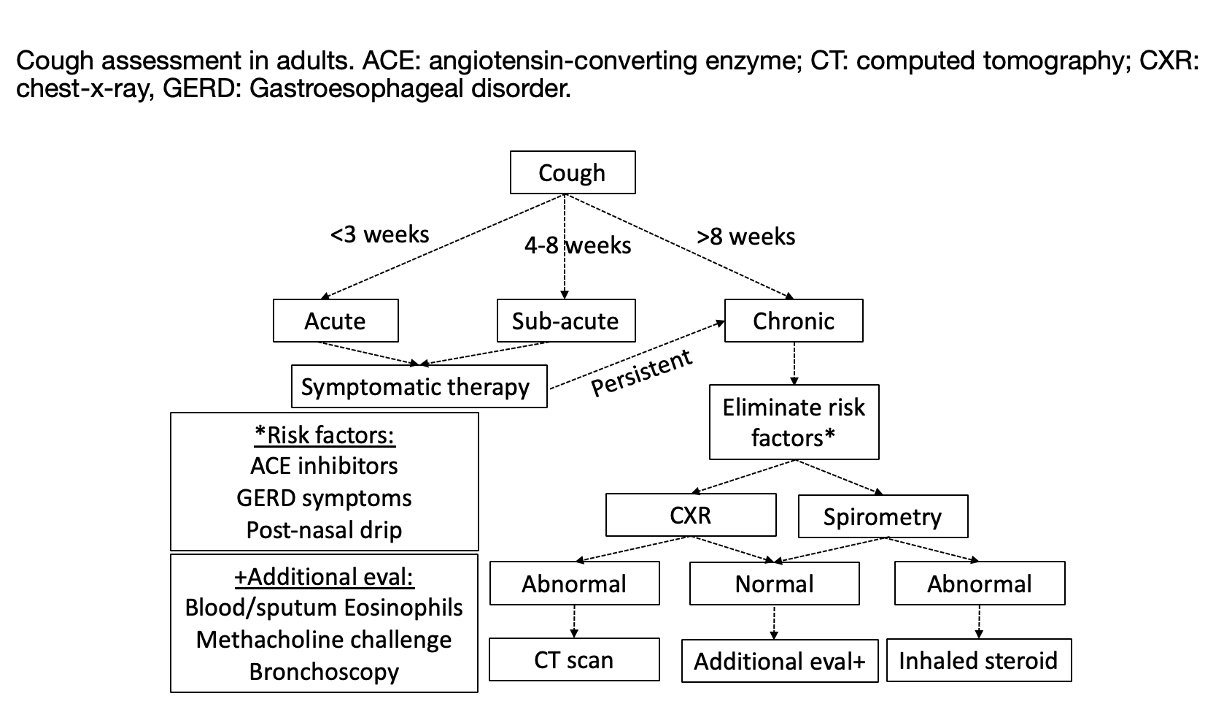
Kastelik JA, Aziz I, Ojoo JC, Thompson RH, Redington AE, Morice AH. Investigation and management of chronic cough using a probability-based algorithm. The European respiratory journal. 2005 Feb:25(2):235-43
[PubMed PMID: 15684286]
[56]
Côté A, Russell RJ, Boulet LP, Gibson PG, Lai K, Irwin RS, Brightling CE, CHEST Expert Cough Panel. Managing Chronic Cough Due to Asthma and NAEB in Adults and Adolescents: CHEST Guideline and Expert Panel Report. Chest. 2020 Jul:158(1):68-96. doi: 10.1016/j.chest.2019.12.021. Epub 2020 Jan 20
[PubMed PMID: 31972181]
[57]
Brightling CE, Ward R, Goh KL, Wardlaw AJ, Pavord ID. Eosinophilic bronchitis is an important cause of chronic cough. American journal of respiratory and critical care medicine. 1999 Aug:160(2):406-10
[PubMed PMID: 10430705]
[58]
Sadeghi MH, Wright CE, Hart S, Crooks M, Morice A. Phenotyping patients with chronic cough: Evaluating the ability to predict the response to anti-inflammatory therapy. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology. 2018 Mar:120(3):285-291. doi: 10.1016/j.anai.2017.12.004. Epub
[PubMed PMID: 29508715]
[59]
Morice AH, Menon MS, Mulrennan SA, Everett CF, Wright C, Jackson J, Thompson R. Opiate therapy in chronic cough. American journal of respiratory and critical care medicine. 2007 Feb 15:175(4):312-5
[PubMed PMID: 17122382]
[60]
Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2012 Nov 3:380(9853):1583-9. doi: 10.1016/S0140-6736(12)60776-4. Epub 2012 Aug 28
[PubMed PMID: 22951084]
Level 1 (high-level) evidence
[61]
Vertigan AE, Kapela SL, Ryan NM, Birring SS, McElduff P, Gibson PG. Pregabalin and Speech Pathology Combination Therapy for Refractory Chronic Cough: A Randomized Controlled Trial. Chest. 2016 Mar:149(3):639-48. doi: 10.1378/chest.15-1271. Epub 2016 Jan 12
[PubMed PMID: 26447687]
Level 1 (high-level) evidence
[62]
Kahrilas PJ, Howden CW, Hughes N, Molloy-Bland M. Response of chronic cough to acid-suppressive therapy in patients with gastroesophageal reflux disease. Chest. 2013 Mar:143(3):605-612. doi: 10.1378/chest.12-1788. Epub
[PubMed PMID: 23117307]
[63]
Berkhof FF, Doornewaard-ten Hertog NE, Uil SM, Kerstjens HA, van den Berg JW. Azithromycin and cough-specific health status in patients with chronic obstructive pulmonary disease and chronic cough: a randomised controlled trial. Respiratory research. 2013 Nov 14:14(1):125. doi: 10.1186/1465-9921-14-125. Epub 2013 Nov 14
[PubMed PMID: 24229360]
Level 1 (high-level) evidence
[64]
Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan:129(1 Suppl):63S-71S. doi: 10.1378/chest.129.1_suppl.63S. Epub
[PubMed PMID: 16428694]
Level 1 (high-level) evidence
[65]
Wakwaya Y, Ramdurai D, Swigris JJ. Managing Cough in Idiopathic Pulmonary Fibrosis. Chest. 2021 Nov:160(5):1774-1782. doi: 10.1016/j.chest.2021.05.071. Epub 2021 Jun 23
[PubMed PMID: 34171385]
[66]
Brown KK. Chronic cough due to chronic interstitial pulmonary diseases: ACCP evidence-based clinical practice guidelines. Chest. 2006 Jan:129(1 Suppl):180S-185S. doi: 10.1378/chest.129.1_suppl.180S. Epub
[PubMed PMID: 16428708]
Level 1 (high-level) evidence
[67]
Gibson P, Wang G, McGarvey L, Vertigan AE, Altman KW, Birring SS, CHEST Expert Cough Panel. Treatment of Unexplained Chronic Cough: CHEST Guideline and Expert Panel Report. Chest. 2016 Jan:149(1):27-44. doi: 10.1378/chest.15-1496. Epub 2016 Jan 6
[PubMed PMID: 26426314]
[68]
Vertigan AE, Theodoros DG, Gibson PG, Winkworth AL. Efficacy of speech pathology management for chronic cough: a randomised placebo controlled trial of treatment efficacy. Thorax. 2006 Dec:61(12):1065-9
[PubMed PMID: 16844725]
Level 1 (high-level) evidence
[69]
Chamberlain S, Garrod R, Birring SS. Cough suppression therapy: does it work? Pulmonary pharmacology & therapeutics. 2013 Oct:26(5):524-7. doi: 10.1016/j.pupt.2013.03.012. Epub 2013 Mar 21
[PubMed PMID: 23524013]
[70]
Ryerson CJ, Abbritti M, Ley B, Elicker BM, Jones KD, Collard HR. Cough predicts prognosis in idiopathic pulmonary fibrosis. Respirology (Carlton, Vic.). 2011 Aug:16(6):969-75. doi: 10.1111/j.1440-1843.2011.01996.x. Epub
[PubMed PMID: 21615619]
[71]
Koskela HO, Lätti AM, Purokivi MK. Long-term prognosis of chronic cough: a prospective, observational cohort study. BMC pulmonary medicine. 2017 Nov 21:17(1):146. doi: 10.1186/s12890-017-0496-1. Epub 2017 Nov 21
[PubMed PMID: 29162060]
[72]
Yousaf N, Montinero W, Birring SS, Pavord ID. The long term outcome of patients with unexplained chronic cough. Respiratory medicine. 2013 Mar:107(3):408-12. doi: 10.1016/j.rmed.2012.11.018. Epub 2012 Dec 19
[PubMed PMID: 23261310]
[73]
Birring SS, Murphy AC, Scullion JE, Brightling CE, Browning M, Pavord ID. Idiopathic chronic cough and organ-specific autoimmune diseases: a case-control study. Respiratory medicine. 2004 Mar:98(3):242-6
[PubMed PMID: 15002760]
Level 2 (mid-level) evidence
[74]
Waring G, Kirk S, Fallon D. The impact of chronic non-specific cough on children and their families: A narrative literature review. Journal of child health care : for professionals working with children in the hospital and community. 2020 Mar:24(1):143-160. doi: 10.1177/1367493518814925. Epub 2019 Jan 3
[PubMed PMID: 30606033]
[75]
Mathur A, Liu-Shiu-Cheong PSK, Currie GP. The management of chronic cough. QJM : monthly journal of the Association of Physicians. 2019 Sep 1:112(9):651-656. doi: 10.1093/qjmed/hcy259. Epub
[PubMed PMID: 30380127]
[77]
Song DJ, Song WJ, Kwon JW, Kim GW, Kim MA, Kim MY, Kim MH, Kim SH, Kim SH, Kim SH, Kim ST, Kim SH, Kim JK, Kim JH, Kim HJ, Kim HB, Park KH, Yoon JK, Lee BJ, Lee SE, Lee YM, Lee YJ, Lim KH, Jeon YH, Jo EJ, Jee YK, Jin HJ, Choi SH, Hur GY, Cho SH, Kim SH, Lim DH. KAAACI Evidence-Based Clinical Practice Guidelines for Chronic Cough in Adults and Children in Korea. Allergy, asthma & immunology research. 2018 Nov:10(6):591-613. doi: 10.4168/aair.2018.10.6.591. Epub
[PubMed PMID: 30306744]
Level 1 (high-level) evidence