Continuing Education Activity
Dental infections, while relatively straightforward regarding diagnosis and access, can be challenging to manage acutely. Dental abscesses or periapical infections typically arise secondary to dental caries (tooth rot related to poor dental hygiene), trauma, or failed dental root canal treatment. Left untreated these infections can be not only extremely painful but also pose a significant risk of descending into the deep neck space or ascending to intracranial sinuses. Identifying, treating and educating patients about a dental abscess will not only grant symptomatic relief but can also prevent dangerous complications. This activity explains when this condition should be considered on differential diagnosis, articulates how to properly evaluate for this condition, and highlights the role of the interprofessional team in caring for patients with this condition.
Objectives:
- Describe the etiologies that can lead to the formation of a dental abscess.
- Summarize the examination and evaluation process for dental abscess, including any necessary diagnostic imaging.
- Review the various antibiotic regimens recommended for treating a dental abscess.
- Explain possible interprofessional team strategies for improving care coordination and communication to advance the evaluation and treatment of dental ascess and improve outcomes.
Introduction
Dental infections, while relatively straightforward regarding diagnosis and access, can be challenging to manage acutely. Dental abscesses or periapical infections typically arise secondary to dental caries (tooth rot related to poor dental hygiene), trauma, or failed dental root canal treatment. Left untreated these infections can be not only extremely painful but also pose a significant risk of descending into the deep neck space or ascending to intracranial sinuses. Identifying, treating and educating patients about a dental abscess will not only grant symptomatic relief but can also prevent dangerous complications.[1][2]
Etiology
Dental caries, dental trauma, and poor dental hygiene are the most frequent causes of a dental abscess. Break down in the protective enamel of teeth allows for oropharyngeal bacteria to enter the tooth cavity (pulp cavity) causing a local infection. As this infection within the pulp cavity grows within the limited space of the tooth, it compresses the inner dentine walls causing severe pain. This infection then tracks down through the root canal and inferiorly into the mandible or superiorly into the maxilla depending on the location of the infected tooth. Another cause that predisposes individuals to a dental abscess is a partially erupted tooth, most commonly a wisdom tooth, where bacteria get trapped between the crown and soft tissues causing inflammation. Other causes include genetic causes such as amelogenesis imperfect that predispose individuals to weakened enamel, more susceptible to wear. Mechanical causes tooth grinding breaks down tooth enamel. Medical conditions like Sjogren syndrome the cause dry mouth which accelerates oropharyngeal microbial growth. Chemical irritants such as smoke from methamphetamine, immunosuppression arising from chemotherapy, or chronic immunosuppressive medical conditions such as HIV/AIDs can predispose individuals to dental caries.[3][4]
Epidemiology
Dental caries and poor dental health are quite common in the United States. Data from the National Health and Nutrition Examination Survey from 2011 to 2012 conducted by the National Center for Health Statistics for dental caries and tooth loss report that 91% of adults aged 20 to 64 had dental caries. These rates were lower for Hispanic, non-Hispanic black Americans, and non-Hispanic Asian adults when compared with non-Hispanic white adults (Dye et al. 2012). Approximately, 27% of adults aged 20 to 64 have untreated tooth decay. Rates of untreated tooth decay were higher in Hispanics at 36% and non-Hispanic Black Americans at 42% (Dye et al. 2012). In adults over age 65, approximately 19% had untreated dental caries (Dye et al. 2012).
A dental abscess and dental-related hospital emergency room (ER) visits are quite common. One study found that dental infection admissions in hospitals occurred at the rate of 1 per 2600 per population in the United States (Wang et al., 2005). The rates for pediatric ER visits are significantly higher for a dental abscess at 47 % (Graham et al., 2000).
This data is not only suggestive of the very high prevalence of poor dental health which is a major predisposing factor to developing a dental abscess, but it also shows that there are racial and likely socioeconomic factors at play. Provider practices may shift because of the population, racial distribution, and socioeconomic demographics of the community.[5][6]
Pathophysiology
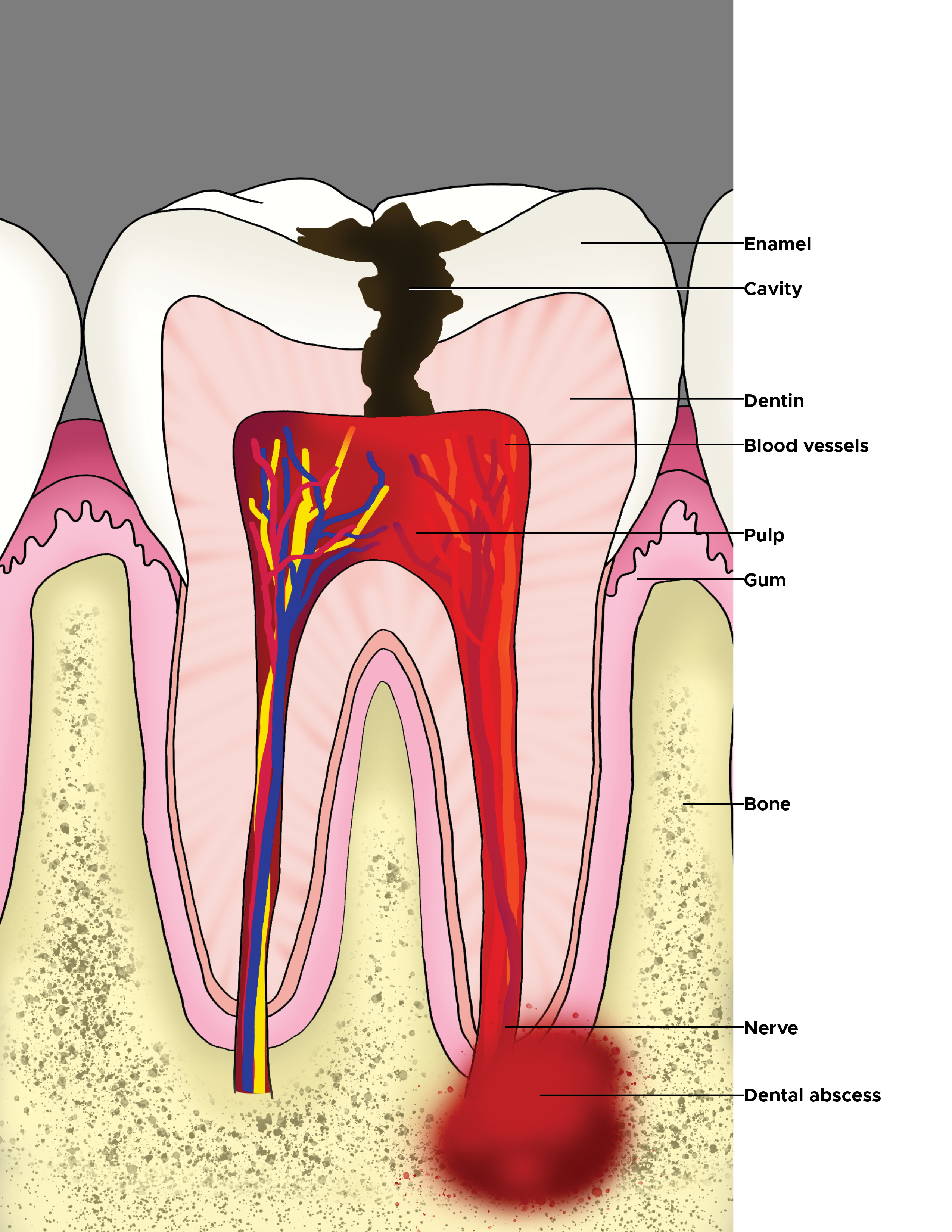
Tooth Anatomy and Structure
The anatomy of the tooth consists of the crown of the tooth which is connected to the root of the tooth which extends into the gum and jaw. The outer most covering of the tooth, the enamel overlays the softer dentine. The nerves and vasculature tunnel through the tooth root canal to the innermost hollow area of the tooth called the pulp canal which houses nerves and vasculature that supply the tooth.
Oral Cavity Flora
The oral cavity is host to many bacteria, mainly gram-negative and facultative anaerobes. These bacteria have varying distribution in the oral cavity; in particular, Streptococcus mitis was found to be most typically found on tooth surfaces (Jorn et al. 2005). This is not always the causative organism in a dental abscess because other oral bacterial species can become introduced into the tooth by other means including but not limited to trauma.
History and Physical
A dental abscess should be considered when patients report severe pain, admit to poor dental hygiene, and lack of adequate dental follow up, admit to dental trauma that was not repaired, localized pain that is reproducible with palpation, facial erythema, trismus, dysphagia, fever, lymphadenopathy. Signs that should immediate illicit concern are altered mental status, dyspnea. When examining the oral cavity, the suspected tooth or teeth harboring infection may be discolored, have visual breaks in the enamel, or be surrounded by gingival erythema and swelling.
Evaluation
CT and MRI are sensitive modalities in detecting abscess. Initial workup should include an x-ray of the head and neck and complete blood cell count. X-ray of head and neck can help identify compression or deviation of the trachea and subcutaneous air related to necrotic tissue. These imaging modalities can be useful if there is a need to evaluate possible ascending bacterial spread to the sinus cavities. Complete blood cell count can help rule in infectious etiology based on total white blood cell count and predominant white blood cell line that appears. For bacterial infections, there should be an increase in neutrophil count in individuals that are not immunocompromised.
Treatment / Management
Treatment involves draining the abscess, providing antibiotic support, pain control and removal of infectious tooth source. Often oral antibiotics with timely dentist appointment for dental carries intervention is sufficient. Dental abscesses may not require an admission to the hospital and administration of intravenous (IV) antibiotics unless the patient presents with worrisome features that include fever, dyspnea or airway compromise secondary to swelling. Most dental abscesses can be treated with antibiotics to cover gram negatives, facultative anaerobes, and strict anaerobes.[1]
Penicillins and cephalosporins can be used in odontogenic infections, but there is increasing antimicrobial resistance due to B-lactamase production. This increase in resistance would make using penicillins in conjunction with other antimicrobials such as metronidazole or an antibiotic with an extended spectrum like ampicillin-sulbactam and ampicillin-clavulanate more appropriate.
- Dosing: Ampicillin-sulbactam 3 g intravenously (IV) every 6 hours
- Dosing: Amoxicillin-clavulanate: 875 mg orally every 12 hours
- Dosing: Penicillin G 2 to 4 IV every four to 6 hours PLUS Metronidazole 500 mg IV or orally every 8 hours
- Dosing: Cefoxitin: 1 to 2 g IV every 4 hours
- Dosing: Cefotetan: 2 g IV every 12 hours
Macrolides should not be used the first line unless the patient has penicillin or cephalosporin allergy. There is increased resistance to macrolides and the bacterial species that exhibit resistance are anaerobic Streptococci and Prevotella species that are major colonizers of the oropharynx and often culprits in a dental abscess.
Metronidazole has excellent coverage against anaerobic organisms but lacks sufficient coverage against aerobic gram-positive organisms. It is recommended to use metronidazole in conjunction with penicillin to extend antimicrobial coverage to include aerobic gram-positive organisms.
- Dosing: Penicillin G 2 to 4 IV every 4 to 6 hours PLUS Metronidazole 500 mg IV or orally every 8 hours
Clindamycin is a good option for patients with allergies to penicillins and cephalosporins. Clindamycin overs coverage against gram-positive organisms, anaerobes, B-lactam resistant organisms and has good bone penetration. It was demonstrated that Clindamycin was equally as effective in treating severe odontogenic infections as Penicillin V (Gilmore et al.).
- Dosing: Clindamycin 600 mg IV every 6 to 8 hours
For severe infections or in immunocompromised patients. Anti-pseudomonal antibiotics like fourth-generation or higher cephalosporins or extended spectrum penicillins like piperacillin-tazobactam should be considered. Carbapenems like meropenem should also be reserved for severe infections. Meropenem has activity against gram-positive and gram-negative organisms as well as resistant organisms.
- Dosing: Piperacillin-tazobactam 4.5 g IV every 6 hours
- Dosing: Meropenem 1 g IV every 8 hours
- Dosing: Cefepime 1 to 2 g IV every 12 hours
Differential Diagnosis
- Langerhans cells histiocytosis
- Periapical granuloma or cyst
Surgical Oncology
Surgical management of a dental abscess can include root canal or tooth extraction. If there is a periapical dental abscess, it may require incision and drainage. Incision and drainage can be performed in the emergency department or the clinic but must be followed up by a dentist.
A root canal is a procedure performed by dentists where the crown of the tooth is removed, revealing the infected tooth roots. These passages are opened with surgical tools and cleaned with a solution. The tooth root is then filled, and the tooth crown is replaced. Complications include breaking surgical tools off inside of tooth root canal, cracked tooth, or incomplete evacuation of bacteria. These complications may require repeat root canal of tooth extraction.
Prognosis
Prognosis for a dental abscess is very good. Prognosis can be quite poor if a dental abscess is left untreated; mortality rate can increase to 40% if patients develop mediastinitis from descending infection (Shweta et al. 2013). Airway compromise may warrant intubation or placement of tracheostomy. Ascending infections through the sinuses or hematogenous spread to the brain increase mortality rate and carry a poor prognosis.
Consultations
For complicated dental abscess, consult maxillofacial surgery or a dentist if there is one on staff.
Enhancing Healthcare Team Outcomes
Patients with a dental abscess usually present with oral cavity pain, fever and difficulty chewing. Healthcare workers outside the dental profession including nurse practitioners should promptly refer these patients to an oral surgeon. Besides antibiotics, most patients also require an initial drainage procedure, to be followed for a formal dental procedure at a later date. For those patients who seek care promptly, the prognosis is good. But any delay in treatment can lead to worsening of the problem and even loss of the tooth.