Introduction
Optic nerve sheath decompression, more commonly known as optic nerve sheath fenestration (ONSF), is a surgical procedure performed to decompress the optic nerves and relieve vision-threatening papilledema in the setting of elevated intracranial pressure (ICP).[1] This procedure is generally considered in cases of pseudotumor cerebri (PTC) syndrome, traumatic optic neuropathy (TON), idiopathic intracranial hypertension (IIH), or other conditions that cause optic nerve compression.[2][3][4][5] See Image. Optic Nerve Sheath Durotomy. ONSF is typically performed in patients experiencing rapid vision loss due to significantly elevated intracranial pressure or in those with progressive visual decline who have not responded to medical therapy or are unable to adhere to treatment. The exact mechanism by which fenestration relieves papilledema is not entirely understood. Both decompression of the perioptic subarachnoid space (SAS) with filtration of cerebrospinal fluid (CSF) out of the SAS through the dural opening, as well as scarring of the surgical site that prevents further accumulation of CSF, are felt to be contributing factors.[6] Optic nerve sheath decompression does not treat the source of the elevated ICP itself, but the procedure does diminish the associated visual sequelae.
With approximately 1 million nerve fibers, the optic nerve conveys visual information from the retina to the brain, rendering it particularly susceptible to compression stresses.[7] The optic nerve consists of intraocular, intraorbital, intracanalicular, and intracranial segments, with the intracanalicular segment being particularly vulnerable to traumatic injury due to its confinement within the bony optic canal.[8] The natural course of optic nerve compression is contingent upon the underlying cause. In instances of TON, commonly linked to craniomaxillofacial injuries, the damage is typically mechanical or ischemic, resulting in partial or total vision loss occurring nearly immediately or within hours of the event.[9] Conversely, diseases such as IIH are characterized by persistent ICP rise, resulting in optic nerve sheath distension, papilledema, and potential vision impairment if left untreated.[10] The underlying cause primarily influences the dissemination patterns in optic nerve compression; for example, severe injuries generally lead to localized injury, whereas disorders associated with elevated ICP might impact the optic nerve bilaterally.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The optic nerve is distinctive among cranial nerves in that it is a central nervous system (CNS) white matter tract that shares a similar developmental origin with the CNS.[11] The optic nerve covering is the same outer connective tissue membrane as the brain: the pia, arachnoid, and dura mater. The pia lies on the brain's surface and follows the brain’s gyri and sulci. The arachnoid mater lies just above the pia mater, and CSF flows in the SAS between the pia and the arachnoid.[12] The dura mater is a strong connective tissue covering that overlies the other arachnoid and pia mater, encasing the brain and spinal cord.[13] The SAS of the optic nerve is contiguous with that of the brain via the suprasellar cistern, allowing the circulation of CSF between the intracranial SAS and the optic nerves in a 3-compartment system. As a result, increases in ICP can be transmitted to the optic nerves and cause optic disc edema, known in this clinical setting as papilledema. ONSF is a surgical procedure to relieve perioptic pressure in elevated ICP-causing papilledema.
The SAS of the human optic nerve is not homogenous; still, it possesses a complex system of arachnoid trabeculae and septa that subdivide the SAS between the arachnoid and pia mater. The trabeculae, septa, and pillars vary in density and arrangement depending upon their specific location within the different portions of the optic nerve. They appear to be more densely and tightly packed in the immediate retrobulbar segment of the optic nerve than in the more distal midorbital and canalicular segments. This variability may play a role in the CSF dynamics between the SAS of the optic nerve and the suprasellar cistern that connects it to the intracranial space and may contribute to the understanding of the pathophysiology of papilledema and the sometimes variable response seen to ONSF.[14]
ICP can result from a multitude of CNS disease states, including intracranial hypertension, venous sinus thrombosis, CNS infections, inflammatory diseases, subarachnoid hemorrhage, and intracranial malignancies or other lesions causing obstructive hydrocephalus.[15][16] Vision loss in the setting of papilledema is thought to occur as a result of the disruption of axonal transport and intraneuronal ischemic damage to the optic nerve.[17][18] An increase in CSF pressure increases tissue pressure on the optic nerve axons, disrupting the gradient between intraocular and retrolaminar pressure, resulting in defective axonal transport, followed by intraaxonal swelling, which is seen as papilledema.[19] This swelling can secondarily compress small arterioles to the nerve, causing intraneuronal ischemia. Clinically, this manifests as vision loss, initially as blind spot enlargement, followed by loss of peripheral and then central vision and field loss. Ultimately, optic nerve atrophy ensues in the setting of chronically elevated ICP and papilledema, often with profound vision loss.
Indications
Indications for ONSF
ONSF is indicated in the setting of vision loss due to elevated ICP, which causes papilledema. Increased ICP can result from a multitude of CNS disease states. The most common of these include PTC syndrome, cerebral venous sinus thrombosis, and intracranial tumors, which cause ICP elevation from decreased CSF outflow. Other, less common, and historical indications are also discussed.
Optic nerve compression causes can be classified into traumatic, nontraumatic, and idiopathic categories.[20] TON arises from blunt or penetrating trauma to the optic nerve, frequently caused by motor vehicle collisions, falls, or sports-related injuries.[21] Direct injury may occur from fracture fragments or hematoma exerting pressure on the optic nerve within the optic canal. Indirect injuries involve kinetic energy transfer to the optic nerve via the skull or orbital structures, resulting in shearing, ischemia, and subsequent inflammation. IIH, previously referred to as PTC, is a significant cause of optic nerve compression, primarily impacting obese women of reproductive age. The pathogenesis entails elevated ICP in the absence of identifiable anatomical brain anomalies.[22] Contributing factors to this illness encompass obesity, specific drugs (such as tetracyclines and retinoids), and hormonal abnormalities. Elevated CSF pressure, if left untreated, may result in chronic papilledema and subsequent optic nerve injury. Elevated ICP can induce vision loss due to defective axonal transport, causing intraaxonal swelling and intraneuronal ischemia. Nontraumatic reasons include tumors, cysts, or vascular lesions that apply pressure on the optic nerve. Neoplasms such as meningiomas or gliomas may originate from the optic nerve or nearby tissues, including the optic chiasm.[23] Vascular abnormalities, such as aneurysms or arteriovenous malformations, can induce compression through direct impingement or hemorrhagic consequences.[24] Additionally, inflammatory or infectious conditions such as optic neuritis or orbital cellulitis may also lead to optic nerve impairment.
PTC Syndrome (IIH)
ONSF is most frequently performed in the setting of PTC, also known as benign intracranial hypertension—a syndrome of elevated ICP without an underlying CNS pathology. IIH is a subset of PTC syndrome in which no secondary cause (eg, transverse sinus stenosis, venous sinus thrombosis, corticosteroid use, or hormonal abnormality) is present. IIH most commonly presents in women of childbearing age who are obese or have recently gained weight. Patients commonly present with symptoms of elevated ICP, including headaches and pulsatile tinnitus, as well as visual symptoms of transient visual obscurations and diplopia from unilateral or bilateral cranial nerve (CN) VI palsies.[25] Severe visual loss from progressive field constriction is typically a late finding associated with significantly elevated ICP and can lead to blindness in 5% of patients.[18] Noninvasive treatment measures include weight loss, acetazolamide, and furosemide.
Diagnostic criteria for IIH in adults and children were revised in 2013 by Friedman et al.[26] Definitive IIH is based on the following criteria:
- Papilledema
- Normal neurologic exam, except for cranial neuropathies
- Neuroimaging that shows 1 or more of the following:
- Typical female patient with obesity: Magnetic resonance imaging (MRI) shows normal brain parenchyma and no meningeal enhancement without hydrocephalus, masses, or structural lesions on magnetic resonance imaging (MRI)
- Other types of patients: Normal MRI and magnetic resonance venography
- Computed tomography (CT) imaging: May be an option (if an MRI is unavailable or unobtainable)
- Normal CSF composition
- Elevated opening lumbar puncture pressure of greater than 250 mm CSF in adults and >280 mm CSF in children, or 250 mm CSF in a nonsedated or normal-weight child
If papilledema is absent, IIH can be diagnosed in the following situations:
- If 2 to 5 of the above are present, and there is also a unilateral or bilateral CN VI palsy.
- If both papilledema and CN VI palsy are absent, it is suggestive of IIH (but not positively diagnosed).
- If 2 to 5 of the above are present, and the patient has at least 3 of the following on neuroimaging:
- Empty sella
- Flattening of the posterior globe
- Distension of the perioptic SAS with or without a tortuous optic nerve
- Transverse venous sinus stenosis [26]
ONSF is an attempt to preserve visual function in patients with PTC who present with vision-threatening papilledema or who have not responded adequately to or cannot tolerate maximal medical therapy. This procedure is an essential tool in the acute setting for patients presenting with “malignant” PTC (extremely high opening pressure, evidence of optic neuropathy, and poor prognosis if treated with medical therapy alone).[25] Serial lumbar punctures (LP) are not recommended to reduce ICP in this clinical setting, given the rapid reaccumulation of CSF and return of elevated ICP. CSF diversion procedures in the form of ventriculoperitoneal shunting or lumboperitoneal shunting can also be used to decrease ICP. While they can effectively reduce papilledema and prevent vision loss, there is the attendant risk of brain and spinal surgery and the not-uncommon complication of shunt failure. ONSF and CSF diversion procedures may both be necessary for patients with malignant PTC syndrome, as well as those with severe vision loss and ICP elevation in PTC refractory to conservative management.
Unilateral ONSF can result in papilledema resolution in both eyes; however, in most cases of severe papilledema and vision loss, bilateral ONSF is required. A review of unilateral ONSF shows that the unfenestrated eye typically shows less papilledema reduction than the operated eye.[25][27] Some patients may also experience improved headaches, but ONSF is not primarily for this indication. Repeat ONSF may be necessary for patients with recurrent visual disturbance or further visual deterioration after surgery.[28][29] A ventriculoperitoneal shunt is preferable in most cases in this setting; however, scarring of the optic nerve sheath from prior surgery makes repeat fenestration more technically challenging, and there is a potentially higher risk of complications.
Cerebral Vein Thrombosis or Stenosis
Obstruction of venous drainage from the cerebral venous system secondary to thrombosis or stenosis can result in increased ICP and papilledema from decreased CSF outflow.[30] This condition can present very similarly to PTC and IIH but tends to have a more rapid onset and more severe visual loss from significant ICP elevation; it is not limited to the demographics of PTC syndrome and should be suspected in nonobese women or men with symptoms and signs of PTC syndrome. This presents in patients with prothrombotic states, including pregnancy, oral contraceptives, factor V Leiden mutations, factor XII deficiency, G20210A mutations, antithrombin III, and protein S deficiency. Therapies include anticoagulation, stenting, or thrombectomy of the cerebral sinus and CSF diversion procedures. ONSF can also be performed to protect visual function in patients with vision-threatening papilledema. The European Federation of Neurological Sciences (EFNS) 2010 guidelines appropriate ONSF in serial lumbar puncture cases, acetazolamide, and/or ventriculoperitoneal shunting, which do not prevent the progression of visual loss in these conditions.[25][31]
Intracranial Masses
Intracranial masses/tumors create increased ICP primarily by restricting the flow of CSF through the ventricles or the outflow of CSF and blood from the brain via the dural venous sinuses.[32] ONSF is a viable option for patients in whom ICP develops rapidly and causes profound vision loss and in whom complete resection of the mass is not possible, resulting in persistent intracranial hypertension. Performing ONSF can dramatically increase the quality of life in these patients by preserving their vision. Of all indications for ONSF, this has the poorest visual prognosis, as the surgery is generally a therapeutic option in late-stage patients with intracranial illness.
Other Indications for ONSF
Up to 40% of patients with cryptococcal meningitis develop ocular disease. Papilledema is the most common manifestation of CNS infection and may result in profound visual loss for patients who survive. Cryptococcal meningitis usually results in a very high organism burden in the CSF and marked inflammation.[33] This leads to increased ICP from the possible aggregation of cryptococcal capsular polysaccharide and the resulting CSF outflow obstruction through arachnoid granulations.[34] Some clinicians consider early ONSF to be essential to avoid visual impairment. Practicing caution before performing invasive surgical procedures on an infected optic nerve is a reasonable consideration. However, study results show that postoperative orbital infections do not occur even when histopathological studies reveal numerous cryptococci.[35][36] This is true even if ONSF takes place before antifungal medication administration.[25][37] Study results have also shown that patients with papilledema from cryptococcal meningitis should be considered for ONSF early in the course, even if the infection is active in the disease.[25][38]
Cerebral infections that may result in ICP include bacterial, viral, fungal, and parasite agents that induce inflammation, cerebral edema, or obstruction of CSF circulation. Bacterial meningitis, caused by organisms like Streptococcus pneumoniae or Neisseria meningitidis, can induce a robust inflammatory response that enhances vascular permeability, resulting in cerebral edema and compromised CSF absorption.[39][40] Encephalitis, primarily of viral etiology (eg, herpes simplex virus and West Nile virus), causes direct neuronal injury and cerebral edema, potentially increasing ICP. Brain abscesses, typically resulting from bacterial infections from adjacent structures (such as the sinuses or middle ear), create localized collections of pus that exert a mass effect, exacerbating and increasing ICP. Tuberculous meningitis and fungal infections, such as Cryptococcus neoformans in immunocompromised individuals, can lead to persistent meningeal inflammation and hydrocephalus from blocking CSF channels.[41] Parasitic diseases, such as neurocysticercosis (induced by Taenia solium), can result in cyst formation inside brain tissue, leading to localized edema, hydrocephalus, or inflammatory reactions that exacerbate ICP.[42] Under these circumstances, increased ICP presents a significant threat to brain herniation. This situation necessitates immediate medical intervention, including antibacterial agents, corticosteroids, or surgical treatments such as CSF shunting or decompression.
Local Disease of the Optic Nerve
- Traumatic optic neuropathy
- This can cause elevated intraorbital pressure and commonly manifests early as an optic nerve hematoma. TON treatment is controversial, and results from a large prospective study showed no difference in outcomes, whether treatment for TON was with observation, corticosteroids, or optic nerve decompression.[25]
- Optic nerve tumors
- The most common optic nerve tumors are gliomas and meningiomas.[43] Visual improvement with ONSF in patients with meningiomas has mixed results in reported cases. Other optic nerve tumors reported to have visual improvement after ONSF include bilateral infiltration with T-cell non-Hodgkin lymphoma and metastatic breast cancer.[25]
- Optic nerve drusen
Contraindications
ONSF should not be performed in patients on chronic anticoagulation treatment due to the attendant risk of bleeding into the orbit. The procedure should typically be avoided in patients with CNS infections due to the potential for seeding of the orbit with the infectious organism. ONSF is generally not performed in patients with mild or moderate vision loss related to ICP elevation, as they should receive a full trial of medical therapy before considering surgical intervention. While headache relief can result in up to 50% of patients, it is not indicated for managing a headache in patients with PTC syndrome and patients with intracranial elevation without optic disc edema or vision loss.[45]
If possible, patients with active or severe infections of the optic nerve or surrounding structures, such as optic neuritis or endophthalmitis, should avoid this type of surgery to prevent the risk of worsening infection and further damage to the optic nerve. In patients with uncontrolled systemic diseases, such as severe cardiovascular instability or uncontrolled diabetes, the risks of anesthesia and postoperative complications outweigh the potential benefits of optic nerve decompression. Additionally, coagulopathy or disorders that impair blood clotting, such as hemophilia or specific anticoagulant therapies, pose a significant risk for bleeding complications during and after surgery.
In cases where there is a structural mass (eg, brain tumor and aneurysm) causing intracranial hypertension, optic nerve decompression can be contraindicated in select patients, as the mass should be addressed directly rather than simply relieving the pressure on the optic nerve. Furthermore, severe vision loss, where the optic nerve has already undergone irreversible damage, makes the procedure less effective, as decompression may not restore vision if the nerve is no longer functional. Patients with poor surgical candidacy due to factors like advanced age or poor overall health may not benefit from optic nerve decompression, and the risks of surgery may not justify the potential gains. Therefore, careful patient selection and thorough evaluation are essential to determine whether optic nerve decompression is viable.
Technique or Treatment
De Wecker was the first to describe ONSF in 1872. There are several surgical approaches for accessing the orbit for fenestration of the optic nerves; however, the final goal is to create a window or a series of slits in the optic nerve sheath just behind the globe to release CSF under pressure causing compression of the nerve. Ophthalmologists typically perform the surgery after training in orbital surgery and/or neuroophthalmology. Based on a 2015 survey of ophthalmologists who perform ONSF, the 3 most commonly used surgical approaches are the medial transconjunctival approach (59%), the superomedial lid crease incision (31%), and lateral orbitotomy (10%).[46] The choice of surgical procedure employed is surgeon-specific, depending on individual surgical training and comfort level with their chosen technique.
All procedures are performed under general anesthesia and magnification, with loupes or a surgical microscope. Surgical preparation and draping should be the usual for ophthalmic plastic surgery. Avoiding injury to the posterior ciliary arteries that course along the surface of the optic nerve sheath and supply the optic nerve and choroid is critical in preventing ischemic optic neuropathy or choroidal infarction.
Medial Transconjunctival Approach
First described in 1973 by Galbraith and Sullivan, the medial transconjunctival approach is the most widely used for exposure and fenestration of the optic nerve.[47] One significant benefit of this approach is that it offers quick access to the retroorbital optic nerve without creating an incision in the skin. However, this approach requires disinsertion of the medial rectus muscle, which can result in postoperative strabismus and diplopia.[48]
- Technique:
- A lid speculum is placed after general anesthesia, and patient preparation is established. A limbal peritomy is made nasally, and dissection is performed down to the bare sclera, where the medial rectus muscle is identified. The medial rectus muscle is isolated with muscle hooks and secured with a 6-0 double-armed polyglactin at the insertion. The muscle is transected from the globe anterior to the suture. A traction suture may be passed through the muscle stump at the insertion so that the globe may be abducted for enhanced exposure. Continuous attention to pupil size and reaction to light is critical in monitoring optic nerve integrity throughout the rest of the procedure. Gentle blunt dissection is carried down along the medial aspect of the globe and into the intraconal space using the surgeon’s orbital retractor of choice.
- Once the optic nerve is visualized, the operating microscope is brought over the field. Fine, long forceps, such as a myringotomy or bayonet, are used to grasp the optic nerve sheath. Sharp scissors are used to incise the optic nerve sheath at least 1 mm away from the nerve insertion. Alternatively, a long fine-cutting instrument, such as a sharp paracentesis knife, may make the first cut. A gush of CSF indicates successful full-thickness penetration of the sheath. Additional cuts with the scissors are made until a tissue window is excised and removed. All orbital instruments are removed, and the medial rectus muscle is reattached at its insertion. Hemostasis is confirmed, and the conjunctiva is closed with the surgeon’s suture of preference.
Farris and Lai described an alternative to this procedure in 2014; their approach entails a transconjunctival approach to the medial intraconal space. Instead of detaching the medial rectus muscle, this muscle and the superior rectus are engaged on bridle sutures used to rotate the globe inferiorly and temporally. The orbit is then entered with an orbital retractor in the space between these muscles to access and fenestrate the optic nerve, as described above.
Superomedial Lid Crease Incision
Pelton and Patel described this surgical approach in 2001.[49] Historically, orbital surgeons have extensively used this approach to access the medial intraconal space to remove intraorbital lesions. By creating the incision in the crease of the upper eyelid, the scar is well-hidden and is appealing to some patients for cosmetic considerations. Some orbital surgeons favor it because the procedure can be performed more quickly than the classical medial transconjunctival approach, affords a direct angle of approach to the optic nerve, and does not require disinsertion of any extraocular muscles. Additionally, an operative microscope is usually unnecessary due to the more direct approach to the nerve than the medial orbitotomy approach. The dissection occurs medially to the levator aponeurosis and optic nerve; as such, there is little danger of ptosis, ciliary ganglion injury, or strabismus. The constraining factor with this approach is the increased distance from the incision site to the optic nerve, and it is relatively more technically challenging to perform.[46]
- Technique:
- The lid crease is marked, and a local anesthetic with epinephrine is injected subcutaneously. After establishing general anesthesia and patient preparation, an incision is made through the medial one-half to two-thirds of the crease over the previously made marking. Sharp dissection is carried through the orbicularis and the septum with cutting cautery or Wescott scissors. The nasal and central (preaponeurotic) fat pads are identified, and careful blunt dissection is performed between them into the orbit between the levator aponeurosis and the superior oblique muscle. Dissection is carried out inferiorly and posteriorly toward the back of the globe in the loose areolar orbital fat until the optic nerve is strummed and then visualized. Continuous attention to pupil size and reaction to light is critical for monitoring optic nerve integrity throughout the rest of the procedure. Neurosurgical cottonoids may then be used to pack around the nerve.
- An operating microscope may be brought over the field per surgeon preference, or loupes may be used for magnification. A fine, long forceps, such as a myringotomy or bayonet, is used to grasp the optic nerve sheath. An incision is then made in the optic nerve sheath at least 1 mm away from the nerve insertion using the surgeon’s instrument of choice, taking care to avoid contact with the nerve itself. A gush of CSF indicates successful full-thickness penetration of the sheath. Additional cuts with the scissors are made until a tissue window is excised and removed. Hemostasis is confirmed, and all instruments are removed from the orbit. The skin is closed with 6-0 plain gut sutures.
Lateral Orbitotomy Approach
This approach was first described for use in ONSF in 1872 by De Wecker and then subsequently in 1988 by Tse et al and Patel and Anderson, who performed the lateral approach without removing the lateral orbital wall.[50] The benefits include an excellent perpendicular view of the optic nerve without requiring muscle disinsertion. However, this approach can increase operating times and injury to the ciliary ganglion. Additionally, an external incision is required.[51]
- Technique:
- After the establishment of general anesthesia and patient preparation, a lateral canthotomy with cantholysis is performed. A traction suture is placed through the cut edge of the upper eyelid and the lid margin. This process is repeated for the lower eyelid. Finally, a third traction suture can be placed at the insertion of the lateral rectus muscle. The globe is adducted using the traction suture. The conjunctiva is incised with Wescott scissors as far laterally as possible so as not to injure the lacrimal gland or lateral rectus muscle belly. Blunt dissection with small malleables is performed between the lacrimal gland and the lateral rectus muscle, directed posterior to the globe. Often, it is necessary to cut through any intermuscular septa that may be present before the intraconal compartment becomes accessible. Blunt dissection is continued through the intraconal fat until the optic nerve is identified. Neurosurgical cottonoids may then be used to pack around the nerve.
- As the focus shifts to the optic nerve, an operating microscope may be brought over the field per surgeon preference, or loupes may be utilized for magnification. A fine, long forceps, such as a myringotomy or bayonet, is used to grasp the optic nerve sheath. An incision is then made in the optic nerve sheath at least 1 mm away from the nerve insertion using the surgeon’s instrument of choice, taking care to avoid contact with the nerve itself. A gush of CSF indicates successful full-thickness penetration of the sheath. Additional cuts with the scissors are made until a tissue window is excised and removed. Hemostasis is confirmed, and the canthotomy and skin are closed using the surgeon’s preferred technique.
A revised lateral approach is another technique that obviates the need to traverse the intraconal fat by following the curve of the globe with the posterior dissection. In this way, it is similar to the medial transconjunctival approach but takes advantage of the additional space afforded by the anatomy.[52]
Endoscopic Nasal Approach
The endoscopic endonasal approach for ONSF is a minimally invasive surgical method that provides direct access to the optic nerve in the medial orbit via the nasal canal.[53] This technique serves as an alternative to conventional transorbital or lateral orbitotomy approaches, which are especially beneficial for patients with IIH or PTC who have not responded to medical treatment and are at risk of irreversible vision loss. The process uses the inherent anatomical pathways of the nasal cavity and paranasal sinuses, circumventing external incisions and minimizing the danger of postoperative scarring, infection, and problems related to transorbital methods.
Using a rigid endoscope, commonly 0-degree or 30-degree high-definition endoscopes, the surgeon attains a magnified, well-illuminated perspective of the optic nerve and its adjacent tissues, facilitating accurate maneuverability. Furthermore, intraoperative navigation tools and imaging guidance mitigate risks by offering real-time localization of essential anatomical landmarks, including the optic canal, carotid artery, and sphenoid sinus. The endoscopic procedure is especially advantageous for patients with considerable orbital fat herniation, prior orbital surgeries, or anatomical changes that complicate conventional ONSF methods. This technique minimizes orbital damage and excessive manipulation of periorbital tissues, perhaps resulting in expedited recovery and less postoperative inflammation, hence becoming a favored option for some patients.[54]
- Technique:
- The endoscopic endonasal ONSF technique commences with the patient placed in a supine position under general anesthesia.[55] The surgical team uses topical vasoconstrictors, such as oxymetazoline or epinephrine-soaked pledgets, to achieve sufficient nasal decongestion, enhancing visualization and reducing intraoperative hemorrhage. Injection of a combined local anesthetic and vasoconstrictive agent into the sphenopalatine area is the most effective way to achieve regional hemostasis. A rigid endoscope is introduced into the nasal cavity, facilitating direct observation of the operative area. The treatment continues with a partial medial turbinectomy or ethmoidectomy, if required, to enhance exposure and promote access to the sphenoid sinus. The sphenoidotomy is meticulously executed via a combination of microdebriders and rongeurs, enabling access to the opticocarotid recess, the principal landmark for locating the optic canal.
- Upon exposure of the optic nerve, meticulous microdissection is conducted using microsurgical instruments to access the optic nerve sheath. A longitudinal incision is performed in the dura of the optic nerve sheath with a small microblade or microscissors, facilitating controlled CSF draining to alleviate pressure. This procedure must be performed with meticulous accuracy to prevent damage to the optic nerve fibers while guaranteeing effective decompression. Hemostasis is preserved during the process using bipolar electrocautery and hemostatic substances. The surgical site is then irrigated, and a little fat graft or hemostatic packing may be used to avert CSF leakage. The nasal mucosa is subsequently adjusted, and meticulous endoscopic examination confirms the absence of substantial hemorrhage or problems before extubation.
- Postoperatively, patients are continuously followed for visual enhancement, potential CSF leaks, and any indications of infection.[56] The endoscopic technique, characterized by its minimally invasive approach and superior vision, presents a viable alternative to conventional ONSF, especially in instances necessitating bilateral surgery or when transorbital methods are inadvisable.[9]
Complications
ONSF is most commonly performed in the setting of IIH; therefore, most of the data published on postoperative complications and outcomes are in this clinical context. Various complications have been reported, most of which are minor and temporary. There is no published comparison of outcomes and complications between different ONSF techniques.
In 2017, Kalyvas looked at ONSF efficacy, complications, and the associated costs of surgical procedures for IIH. There were 525 ONSF procedures performed on 341 patients, with an average follow-up time of 42.3 months. The medial approach was performed in 342 eyes, the lateral in 53 eyes, combined in 3 eyes, and the superomedial lid incision in 1 eye. The researchers concluded that ONSF could reduce papilledema and improve vision. Disc swelling improved in 95% of patients, visual acuity improved in 67%, and visual fields showed improvement in 64%. However, ONSF was less efficacious in headache relief (41%). Approximately 11% required a second fenestration procedure even after initially improving.[57] In another study, 95% of patients who underwent ONSF had improved visual acuity and visual fields with no reported intraoperative complications. The mean follow-up was 18.7 months, and postoperative complications were ocular misalignment (6%) and corneal dellen (0.8%).[44][58]
Interestingly, results from a retrospective chart review published in 2011 by Alsuhaibani showed bilateral improvement of papilledema and vision with unilateral ONSF.[27][58] A search of the literature on ONSF outcomes for IIH overwhelmingly reveals a marked improvement in patients, greater than 90% in nearly every study, particularly in cases with acute papilledema. Further, in a 2008 prospective study in India that compared ONSF for papilledema from IIH vs cerebral venous thrombosis, there was an improvement in 94% of patients in optic disc edema and vision with minimal and transient complications. These complications included tonic pupil (13.4%), diplopia (3.4%), and orbital cellulitis in 1 patient. Visual worsening was found in 2 eyes at 1 month postoperatively, which failed to improve despite repeat fenestration.[59] Fonseca compared ONSF to CSF diversion procedures and found that CSF shunting was superior to ONSF in terms of visual improvement. However, patients with ONSF in this study had worse preoperative papilledema and visual acuity. No complications were reported, but 21% of the patients with ONSF eventually required CSF shunting.[58][60]
Results from additional studies on repeat fenestrations for papilledema also show significant improvement in visual function despite requiring multiple surgeries. Two studies published in 1991 looked at repeat ONSF procedures. In Kelman's study, 12 patients required repeated decompression with concurrent functioning lumboperitoneal shunts. All 12 patients showed improvement in visual function without surgical complications.[61] Spoor studied 13 of 53 IIH individuals with acute papilledema and visual loss who recently underwent ONSF. Eleven of 13 patients showed visual improvement even after secondary or tertiary decompressions.[58][62]
Visual outcomes typically worsen with prolonged exposure to elevated intracranial pressure on the optic nerve, leading to irreversible axonal function loss. The earlier the intervention can be instituted to prevent progressive vision loss, the better. Although not employed solely to treat headaches, ONSF may reduce headaches in over half of patients with IIH undergoing the procedure.[29][45] The mechanism for the improvement of headaches after ONSF is unclear.
The most feared and serious complication of ONSF is complete visual loss, which occurs either as a complication of the procedure or as a therapeutic failure of an uncomplicated fenestration despite improvement of the appearance of the optic nerve. The risk of blindness from ONSF is rare and reportedly 1% to 2% based on large cohort studies.[63][64] Blindness can result from damage to the posterior ciliary arteries, leading to arterial occlusion and choroid or optic nerve ischemia, or from orbital conditions such as retrobulbar hemorrhage or hematoma, which compress the optic nerve or increase intraocular pressure.
Optic nerve sheath cysts and pseudomeningocele have also developed after ONSF and can present with postoperative vision changes, pain, and proptosis.[65] Ptosis, strabismus, or ciliary ganglion injury may also occur; however, the deficits related to these occurrences are often transient and minimal and are related to the surgical approach used for ONSF. The medial transconjunctival approach requires detachment of the medial rectus, which can result in exotropia and diplopia; however, the double vision is typically transient. Due to the proximity of the posterior ciliary nerves and ciliary ganglion, the medial and lateral approaches may result in a tonic pupil.[63][66] Larger studies are required to determine the incidence of these complications.
Other potential complications of ONSF include the following:
- Conjunctiva and sclera
- Chemosis, globe perforation, conjunctival bleeding
- Cornea
- Corneal dellen, corneal ulceration [67]
- Anterior chamber
- Acute angle-closure glaucoma, microhyphema
- Iris
- Tonic pupil
- Retina and choroid
- Branch retinal artery occlusion, central retinal artery occlusion, choroidal ischemia/infarction, chorioretinal scarring
- Optic nerve
- Optic nerve cysts/pseudo meningocele, traumatic optic neuropathy [68]
- Posterior ciliary nerve and ciliary ganglion
- Diplopia, ptosis, mydriasis
- Orbit
- Orbital apex syndrome, infection, hemorrhage/hematoma
- Extraocular muscles
- Strabismus, diplopia [69]
Considering that visual loss is an infrequent complication, and others are relatively minor and transient, ONSF is an attractive option for treating vision loss in PTC/IIH. This is especially true when considering the risks of alternative treatments, such as CSF diversion procedures and bariatric surgery.
Clinical Significance
ONSF is a surgical procedure to prevent vision loss from papilledema in increased ICP. This procedure is most commonly used to prevent vision loss from papilledema in IIH but has other indications reported in the literature. There are 3 major approaches to exposing the optic nerve for decompression, with the medial transconjunctival approach being the most common. Stability or improvement in visual function is seen in the majority of patients, as is a reduction of papilledema grade. The rate of major complications is relatively low, and many minor complications, such as ptosis and diplopia, are usually transient. Future studies are needed to evaluate other ONSF indications and compare outcomes between different surgical approaches. Comparison studies of ONSF and CSF diversion procedures for treating visual compromise from papilledema will also be beneficial, and a major study is currently in the planning stages.
Enhancing Healthcare Team Outcomes
Caring for patients requiring optic nerve decompression—whether due to traumatic optic neuropathy, compressive lesions, or conditions such as IIH—demands advanced surgical skills, strategic decision-making, and precise interprofessional coordination. Prolonged optic nerve compression caused by significantly elevated intracranial pressure can lead to irreversible ischemic injury. Optic nerve sheath fenestration, a key intervention in papilledema and malignant pseudotumor cerebri cases, has shown greater success when performed early. Clinicians must adeptly identify signs such as optic disc edema and peripheral visual field constriction, and be prepared to initiate timely referrals. Primary care and emergency clinicians, optometrists, and ophthalmologists play vital roles in early detection, appropriate workup, and escalation to surgical management. Radiologists, anesthesiologists, and neuroophthalmologists further contribute to diagnostic clarity, operative planning, and perioperative support. Pharmacists assist in managing adjunctive medications such as corticosteroids or acetazolamide, while nurses provide essential perioperative care and patient education.
Interprofessional communication and strategic care coordination are critical throughout this process. Emergency recognition of elevated ICP and potential vision loss, prompt ophthalmologic evaluation, and appropriate surgical referral—often to experienced orbital or skull base surgeons—are key to optimizing visual outcomes. In some cases, when ONSF is insufficient or contraindicated, neurosurgical involvement for cerebrospinal fluid diversion may be required. Nurses and surgical staff must be familiar with the procedure and prepared to monitor for complications such as cerebrospinal fluid leak, infection, or worsening vision. This collaborative approach enhances patient safety, outcomes, and satisfaction. By adhering to evidence-based protocols, upholding surgical ethics, and embracing multidisciplinary teamwork, clinicians can deliver high-quality, patient-centered care to individuals undergoing optic nerve decompression, maximizing the preservation of visual function and overall neurological stability.
Media
(Click Image to Enlarge)
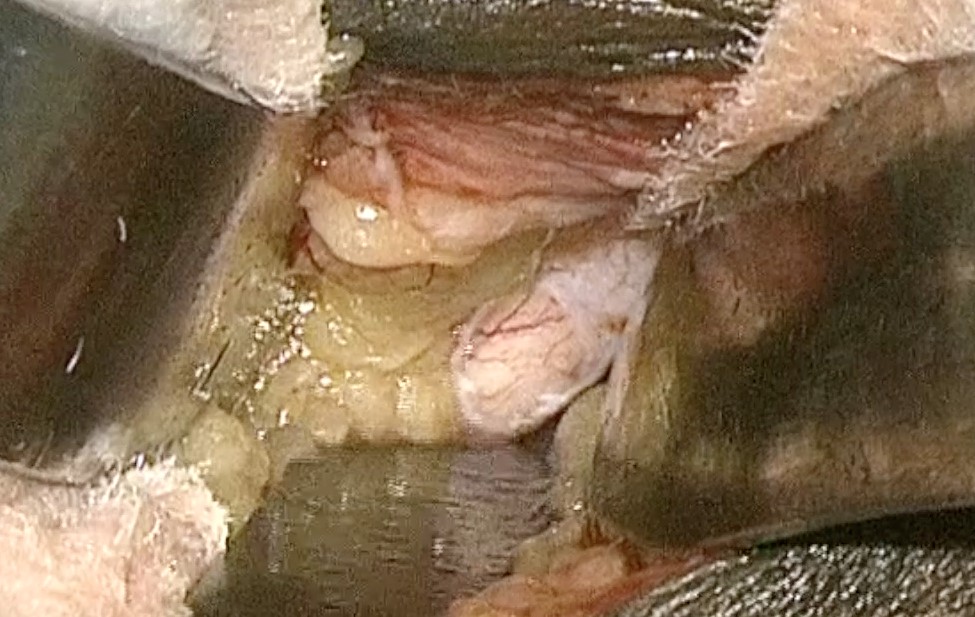
Optic Nerve Sheath Durotomy. This image shows the optic nerve sheath durotomy during an optic nerve fenestration via the lid crease approach.
Contributed by O Adesina, MD
References
Sharma M, Chhabra A, Raina N. Optic nerve sheath fenestration: A second lease at sight. Indian journal of ophthalmology. 2023 Jul:71(7):2845-2849. doi: 10.4103/IJO.IJO_3027_22. Epub [PubMed PMID: 37417132]
Söylev Bajin M, Durmaz Engin C, Yaman A, Ayhan Z, Gökçay F, Çelebisoy N, Men S, Akdal G, Halmágyi GM. Optic nerve sheath decompression saves sight in severe papilloedema: results from 81 eyes in 56 patients with pseudotumor cerebri. Acta ophthalmologica. 2021 Nov:99(7):e991-e998. doi: 10.1111/aos.14732. Epub 2020 Dec 30 [PubMed PMID: 33377617]
Hossain I, Rostami E, Marklund N. The management of severe traumatic brain injury in the initial postinjury hours - current evidence and controversies. Current opinion in critical care. 2023 Dec 1:29(6):650-658. doi: 10.1097/MCC.0000000000001094. Epub 2023 Oct 11 [PubMed PMID: 37851061]
Level 3 (low-level) evidenceCorecha Santos R, Gupta B, Santiago RB, Sabahi M, Kaye B, Dabecco R, Obrzut M, Adada B, Velasquez N, Borghei-Razavi H. Endoscopic endonasal optic nerve sheath decompression (EONSD) for idiopathic intracranial hypertension: Technical details and meta-analysis. Clinical neurology and neurosurgery. 2023 Jun:229():107750. doi: 10.1016/j.clineuro.2023.107750. Epub 2023 Apr 30 [PubMed PMID: 37146367]
Level 1 (high-level) evidenceBasma J, Dacus MR, Kumar R, Spencer D, Arnautović KI. Cisternal, Falciform, and Optic Canal Decompression Influencing Optic Nerve Biomechanics: A Microsurgical Anatomic Study. Operative neurosurgery (Hagerstown, Md.). 2023 Feb 1:24(2):e75-e84. doi: 10.1227/ons.0000000000000472. Epub 2022 Nov 4 [PubMed PMID: 36637310]
Davidson SI. A surgical approach to plerocephalic disc oedema. Transactions of the ophthalmological societies of the United Kingdom. 1970:89():669-90 [PubMed PMID: 5276692]
Freddi TAL, Ottaiano AC. The Optic Nerve: Anatomy and Pathology. Seminars in ultrasound, CT, and MR. 2022 Oct:43(5):378-388. doi: 10.1053/j.sult.2022.04.006. Epub 2022 Apr 13 [PubMed PMID: 36116850]
Robba C, Santori G, Czosnyka M, Corradi F, Bragazzi N, Padayachy L, Taccone FS, Citerio G. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive care medicine. 2018 Aug:44(8):1284-1294. doi: 10.1007/s00134-018-5305-7. Epub 2018 Jul 17 [PubMed PMID: 30019201]
Level 1 (high-level) evidenceSasindran V, John MS. Endoscopic Optic Nerve Decompression for Direct Traumatic Optic Neuropathy : Our 10 Years Experience. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2022 Dec:74(4):594-599. doi: 10.1007/s12070-022-03194-y. Epub 2022 Nov 19 [PubMed PMID: 36514422]
Case D, Seinfeld J, Roark C, Kumpe D. Idiopathic Intracranial Hypertension: Contemporary Management and Endovascular Techniques. Seminars in interventional radiology. 2020 Jun:37(2):175-181. doi: 10.1055/s-0040-1709172. Epub 2020 May 14 [PubMed PMID: 32419730]
Level 3 (low-level) evidenceSonne J, Omole AE, Lopez-Ojeda W. Neuroanatomy, Cranial Nerve. StatPearls. 2025 Jan:(): [PubMed PMID: 29261885]
Durouchoux A, Liguoro D, Sesay M, Le Petit L, Jecko V. Subarachnoid space of the optic nerve sheath and intracranial hypertension: a macroscopic, light and electron microscopic study. Surgical and radiologic anatomy : SRA. 2022 May:44(5):759-766. doi: 10.1007/s00276-022-02948-1. Epub 2022 May 4 [PubMed PMID: 35507023]
Pansell J, Bell M, Rudberg P, Friman O, Cooray C. Optic nerve sheath diameter in intracranial hypertension: Measurement external or internal of the dura mater? Journal of neuroimaging : official journal of the American Society of Neuroimaging. 2023 Jan:33(1):58-66. doi: 10.1111/jon.13062. Epub 2022 Oct 5 [PubMed PMID: 36197323]
Killer HE, Laeng HR, Flammer J, Groscurth P. Architecture of arachnoid trabeculae, pillars, and septa in the subarachnoid space of the human optic nerve: anatomy and clinical considerations. The British journal of ophthalmology. 2003 Jun:87(6):777-81 [PubMed PMID: 12770980]
Hvas CL, Andersen ÅB, Møller K, Hansen K, Poulsen FR, Overgaard-Steensen C. Increased intracranial pressure in acute bacterial meningitis. Ugeskrift for laeger. 2023 Dec 18:185(51):. pii: V06230363. Epub [PubMed PMID: 38105735]
Hawryluk GWJ, Citerio G, Hutchinson P, Kolias A, Meyfroidt G, Robba C, Stocchetti N, Chesnut R. Intracranial pressure: current perspectives on physiology and monitoring. Intensive care medicine. 2022 Oct:48(10):1471-1481. doi: 10.1007/s00134-022-06786-y. Epub 2022 Jul 11 [PubMed PMID: 35816237]
Level 3 (low-level) evidenceRigi M, Almarzouqi SJ, Morgan ML, Lee AG. Papilledema: epidemiology, etiology, and clinical management. Eye and brain. 2015:7():47-57. doi: 10.2147/EB.S69174. Epub 2015 Aug 17 [PubMed PMID: 28539794]
Level 2 (mid-level) evidenceWall M. Idiopathic intracranial hypertension. Neurologic clinics. 2010 Aug:28(3):593-617. doi: 10.1016/j.ncl.2010.03.003. Epub [PubMed PMID: 20637991]
Xie JS, Donaldson L, Margolin E. Papilledema: A review of etiology, pathophysiology, diagnosis, and management. Survey of ophthalmology. 2022 Jul-Aug:67(4):1135-1159. doi: 10.1016/j.survophthal.2021.11.007. Epub 2021 Nov 20 [PubMed PMID: 34813854]
Level 3 (low-level) evidenceAtkins EJ, Newman NJ, Biousse V. Lesions of the optic nerve. Handbook of clinical neurology. 2011:102():159-84. doi: 10.1016/B978-0-444-52903-9.00012-1. Epub [PubMed PMID: 21601066]
Karimi S, Arabi A, Ansari I, Shahraki T, Safi S. A Systematic Literature Review on Traumatic Optic Neuropathy. Journal of ophthalmology. 2021:2021():5553885. doi: 10.1155/2021/5553885. Epub 2021 Feb 26 [PubMed PMID: 33728056]
Level 1 (high-level) evidenceWang MTM, Bhatti MT, Danesh-Meyer HV. Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2022 Jan:95():172-179. doi: 10.1016/j.jocn.2021.11.029. Epub 2021 Dec 17 [PubMed PMID: 34929642]
Al-Bader D, Hasan A, Behbehani R. Sellar masses: diagnosis and treatment. Frontiers in ophthalmology. 2022:2():970580. doi: 10.3389/fopht.2022.970580. Epub 2022 Nov 24 [PubMed PMID: 38983521]
Mattogno PP, Sturiale CL, Rapisarda A, Olivi A, Albanese A. Strategies for Optic Pathways Decompression for Extra-Axial Tumors or Intracranial Aneurysms: A Technical Note. Journal of neurological surgery. Part A, Central European neurosurgery. 2021 Sep:82(5):475-483. doi: 10.1055/s-0040-1720991. Epub 2021 Feb 28 [PubMed PMID: 33641136]
Chen H, Zhang Q, Tan S, Fu H, Farris BK, Yang Z. Update on the application of optic nerve sheath fenestration. Restorative neurology and neuroscience. 2017:35(3):275-286 [PubMed PMID: 28339414]
Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013 Sep 24:81(13):1159-65. doi: 10.1212/WNL.0b013e3182a55f17. Epub 2013 Aug 21 [PubMed PMID: 23966248]
Alsuhaibani AH, Carter KD, Nerad JA, Lee AG. Effect of optic nerve sheath fenestration on papilledema of the operated and the contralateral nonoperated eyes in idiopathic intracranial hypertension. Ophthalmology. 2011 Feb:118(2):412-4. doi: 10.1016/j.ophtha.2010.06.025. Epub [PubMed PMID: 20801522]
Level 2 (mid-level) evidenceBanta JT, Farris BK. Pseudotumor cerebri and optic nerve sheath decompression. Ophthalmology. 2000 Oct:107(10):1907-12 [PubMed PMID: 11013197]
Level 2 (mid-level) evidenceSergott RC, Savino PJ, Bosley TM. Optic nerve sheath decompression: a clinical review and proposed pathophysiologic mechanism. Australian and New Zealand journal of ophthalmology. 1990 Nov:18(4):365-73 [PubMed PMID: 2076284]
M O, Jk CG, I G, Nr K, Cm C, W B. Prevalence of cerebral vein thrombosis among patients with spontaneous intracranial hypotension. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2022 Dec:28(6):719-725. doi: 10.1177/15910199211065912. Epub 2021 Dec 14 [PubMed PMID: 34904470]
Einhäupl K, Stam J, Bousser MG, De Bruijn SF, Ferro JM, Martinelli I, Masuhr F, European Federation of Neurological Societies. EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. European journal of neurology. 2010 Oct:17(10):1229-35. doi: 10.1111/j.1468-1331.2010.03011.x. Epub [PubMed PMID: 20402748]
Sharma S, Hashmi MF, Davidson CL, Kumar A. Intracranial Hypertension. StatPearls. 2025 Jan:(): [PubMed PMID: 29939588]
Tugume L, Ssebambulidde K, Kasibante J, Ellis J, Wake RM, Gakuru J, Lawrence DS, Abassi M, Rajasingham R, Meya DB, Boulware DR. Cryptococcal meningitis. Nature reviews. Disease primers. 2023 Nov 9:9(1):62. doi: 10.1038/s41572-023-00472-z. Epub 2023 Nov 9 [PubMed PMID: 37945681]
Graybill JR, Sobel J, Saag M, van Der Horst C, Powderly W, Cloud G, Riser L, Hamill R, Dismukes W. Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2000 Jan:30(1):47-54 [PubMed PMID: 10619732]
Level 1 (high-level) evidenceMilman T, Mirani N, Turbin RE. Optic nerve sheath fenestration in cryptococcal meningitis. Clinical ophthalmology (Auckland, N.Z.). 2008 Sep:2(3):637-9 [PubMed PMID: 19668765]
Level 3 (low-level) evidenceGarrity JA, Herman DC, Imes R, Fries P, Hughes CF, Campbell RJ. Optic nerve sheath decompression for visual loss in patients with acquired immunodeficiency syndrome and cryptococcal meningitis with papilledema. American journal of ophthalmology. 1993 Oct 15:116(4):472-8 [PubMed PMID: 8213978]
Level 3 (low-level) evidenceTan CT. Intracranial hypertension causing visual failure in cryptococcus meningitis. Journal of neurology, neurosurgery, and psychiatry. 1988 Jul:51(7):944-6 [PubMed PMID: 3204403]
Cremer PD, Johnston IH, Halmagyi GM. Pseudotumour cerebri syndrome due to cryptococcal meningitis. Journal of neurology, neurosurgery, and psychiatry. 1997 Jan:62(1):96-8 [PubMed PMID: 9010409]
Level 3 (low-level) evidenceFarias LABG, Firmino NN, Sousa MM, Lira ML, Meireles LN, Stolp ÂMV, Maia KM, Costa SF, Perdigão Neto LV. Streptococcus constellatus causing concomitant extra and intracranial abscesses complicated with sagittal sinus thrombosis. Revista do Instituto de Medicina Tropical de Sao Paulo. 2023:65():e10. doi: 10.1590/S1678-9946202365010. Epub 2023 Jan 30 [PubMed PMID: 36722672]
El-Hajj VG, Pettersson I, Gharios M, Ghaith AK, Bydon M, Edström E, Elmi-Terander A. Detection and Management of Elevated Intracranial Pressure in the Treatment of Acute Community-Acquired Bacterial Meningitis: A Systematic Review. Neurocritical care. 2024 Aug:41(1):228-243. doi: 10.1007/s12028-023-01937-5. Epub 2024 Feb 14 [PubMed PMID: 38356077]
Level 1 (high-level) evidenceGregoire E, Pirotte BF, Moerman F, Altdorfer A, Gaspard L, Firre E, Moonen M, Darcis G. Mycobacterium avium complex and Cryptococcus neoformans co-infection in a patient with acquired immunodeficiency syndrome: a case report. Acta clinica Belgica. 2022 Jun:77(3):679-684. doi: 10.1080/17843286.2021.1919845. Epub 2021 Apr 22 [PubMed PMID: 33886444]
Level 3 (low-level) evidenceMilenkovic ZJ, Momcilovic SD, Ignjatovic AM, Trenkic-Aracki A, Dzopalic TM, Vidovic NT, Jovic ZK, Tasic-Otasevic SA. Intraventricular Neurocysticercosis: Comparative Analysis of Different Localizations. Clinical Course and Treatment. A Systematic Review. Journal of neurological surgery. Part A, Central European neurosurgery. 2023 Jul 4:():. doi: 10.1055/a-2122-7391. Epub 2023 Jul 4 [PubMed PMID: 37402404]
Level 1 (high-level) evidenceXu D, Zhou J, Mei H, Li H, Sun W, Xu H. Impediment of Cerebrospinal Fluid Drainage Through Glymphatic System in Glioma. Frontiers in oncology. 2021:11():790821. doi: 10.3389/fonc.2021.790821. Epub 2022 Jan 10 [PubMed PMID: 35083148]
Moreau A, Lao KC, Farris BK. Optic nerve sheath decompression: a surgical technique with minimal operative complications. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2014 Mar:34(1):34-8. doi: 10.1097/WNO.0000000000000065. Epub [PubMed PMID: 24275984]
Level 2 (mid-level) evidenceBrazis PW. Clinical review: the surgical treatment of idiopathic pseudotumour cerebri (idiopathic intracranial hypertension). Cephalalgia : an international journal of headache. 2008 Dec:28(12):1361-73. doi: 10.1111/j.1468-2982.2008.01778.x. Epub [PubMed PMID: 19037972]
Sobel RK, Syed NA, Carter KD, Allen RC. Optic Nerve Sheath Fenestration: Current Preferences in Surgical Approach and Biopsy. Ophthalmic plastic and reconstructive surgery. 2015 Jul-Aug:31(4):310-2. doi: 10.1097/IOP.0000000000000326. Epub [PubMed PMID: 26168208]
Galbraith JE, Sullivan JH. Decompression of the perioptic meninges for relief of papilledema. American journal of ophthalmology. 1973 Nov:76(5):687-92 [PubMed PMID: 4748189]
Cruz AAV, Cunha BS. Position of the anterior ethmoidal foramen and trauma to the cranial base during transconjunctival medial orbital decompression: a systematic literature review. Orbit (Amsterdam, Netherlands). 2024 Oct:43(5):674-682. doi: 10.1080/01676830.2023.2274866. Epub 2023 Nov 9 [PubMed PMID: 37942625]
Level 1 (high-level) evidencePelton RW, Patel BC. Superomedial lid crease approach to the medial intraconal space: a new technique for access to the optic nerve and central space. Ophthalmic plastic and reconstructive surgery. 2001 Jul:17(4):241-53 [PubMed PMID: 11476174]
Level 3 (low-level) evidenceTse DT, Nerad JA, Anderson RL, Corbett JJ. Optic nerve sheath fenestration in pseudotumor cerebri. A lateral orbitotomy approach. Archives of ophthalmology (Chicago, Ill. : 1960). 1988 Oct:106(10):1458-62 [PubMed PMID: 3052386]
Hakim SG, Sieg P. Resection of medial orbital tumours via lateral orbitotomy and minimally invasive microscopic, transconjunctival and pre-caruncular approaches. The British journal of oral & maxillofacial surgery. 2022 May:60(4):519-521. doi: 10.1016/j.bjoms.2021.09.002. Epub 2021 Sep 16 [PubMed PMID: 35317938]
Blessing NW, Tse DT. Optic nerve sheath fenestration: a revised lateral approach for nerve access. Orbit (Amsterdam, Netherlands). 2019 Apr:38(2):137-143. doi: 10.1080/01676830.2018.1452949. Epub 2018 Mar 22 [PubMed PMID: 29565728]
Lee IH, Yoon WS, Kim DH, Son SA. Endoscopic Endonasal Optic Nerve Decompression in a Patient With Invasive Fungal Sinusitis Invasion Into the Orbital Apex: Intraoperative Video and Literature Review. The Journal of craniofacial surgery. 2023 Jan-Feb 01:34(1):291-294. doi: 10.1097/SCS.0000000000008882. Epub 2022 Aug 15 [PubMed PMID: 35968978]
Göksu E, Bozkurt B, İlhan D, Özak A, Çırak M, Yağmurlu K. Endoscopic Bilateral Optic Nerve Decompression for Treatment of Idiopathic Intracranial Hypertension. Brain sciences. 2021 Mar 4:11(3):. doi: 10.3390/brainsci11030324. Epub 2021 Mar 4 [PubMed PMID: 33806665]
Cabrilo I, Dorward NL. Endoscopic endonasal intracanalicular optic nerve decompression: how I do it. Acta neurochirurgica. 2020 Sep:162(9):2129-2134. doi: 10.1007/s00701-020-04476-6. Epub 2020 Jul 19 [PubMed PMID: 32686070]
Berhouma M, Jacquesson T, Abouaf L, Vighetto A, Jouanneau E. Endoscopic endonasal optic nerve and orbital apex decompression for nontraumatic optic neuropathy: surgical nuances and review of the literature. Neurosurgical focus. 2014:37(4):E19. doi: 10.3171/2014.7.FOCUS14303. Epub [PubMed PMID: 25270138]
Kalyvas AV, Hughes M, Koutsarnakis C, Moris D, Liakos F, Sakas DE, Stranjalis G, Fouyas I. Efficacy, complications and cost of surgical interventions for idiopathic intracranial hypertension: a systematic review of the literature. Acta neurochirurgica. 2017 Jan:159(1):33-49. doi: 10.1007/s00701-016-3010-2. Epub 2016 Nov 9 [PubMed PMID: 27830325]
Level 1 (high-level) evidenceGilbert AL, Chwalisz B, Mallery R. Complications of Optic Nerve Sheath Fenestration as a Treatment for Idiopathic Intracranial Hypertension. Seminars in ophthalmology. 2018:33(1):36-41. doi: 10.1080/08820538.2017.1353810. Epub [PubMed PMID: 29420144]
Nithyanandam S, Manayath GJ, Battu RR. Optic nerve sheath decompression for visual loss in intracranial hypertension: report from a tertiary care center in South India. Indian journal of ophthalmology. 2008 Mar-Apr:56(2):115-20 [PubMed PMID: 18292621]
Fonseca PL, Rigamonti D, Miller NR, Subramanian PS. Visual outcomes of surgical intervention for pseudotumour cerebri: optic nerve sheath fenestration versus cerebrospinal fluid diversion. The British journal of ophthalmology. 2014 Oct:98(10):1360-3. doi: 10.1136/bjophthalmol-2014-304953. Epub 2014 May 12 [PubMed PMID: 24820047]
Level 2 (mid-level) evidenceKelman SE, Sergott RC, Cioffi GA, Savino PJ, Bosley TM, Elman MJ. Modified optic nerve decompression in patients with functioning lumboperitoneal shunts and progressive visual loss. Ophthalmology. 1991 Sep:98(9):1449-53 [PubMed PMID: 1945323]
Spoor TC, Ramocki JM, Madion MP, Wilkinson MJ. Treatment of pseudotumor cerebri by primary and secondary optic nerve sheath decompression. American journal of ophthalmology. 1991 Aug 15:112(2):177-85 [PubMed PMID: 1867302]
Mudumbai RC. Optic nerve sheath fenestration: indications, techniques, mechanisms and, results. International ophthalmology clinics. 2014 Winter:54(1):43-9. doi: 10.1097/IIO.0000000000000008. Epub [PubMed PMID: 24296370]
Sergott RC, Savino PJ, Bosley TM. Modified optic nerve sheath decompression provides long-term visual improvement for pseudotumor cerebri. Archives of ophthalmology (Chicago, Ill. : 1960). 1988 Oct:106(10):1384-90 [PubMed PMID: 3178549]
Naqvi SM, Thiagarajah C, Golnik K, Lee A, Kersten R, Nerad J. Optic nerve cyst-like formation presenting as a delayed complication of optic nerve sheath fenestration. Ophthalmic plastic and reconstructive surgery. 2014 May-Jun:30(3):e53-4. doi: 10.1097/IOP.0b013e31829bb3e8. Epub [PubMed PMID: 23880976]
Level 3 (low-level) evidenceArai H, Sato K, Katsuta T, Rhoton AL Jr. Lateral approach to intraorbital lesions: anatomic and surgical considerations. Neurosurgery. 1996 Dec:39(6):1157-62; discussion 1162-3 [PubMed PMID: 8938770]
Hainsworth DP, Bierly JR, Schmeisser ET, Baker RS. Corneal topographic changes after extraocular muscle surgery. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1999 Apr:3(2):80-6 [PubMed PMID: 10221799]
Chowdhury HR, Rajak S, Heath D, Brittain P. Optical coherence tomography imaging of the optic nerve head pre optic and post optic nerve sheath fenestration. BMJ case reports. 2015 Jul 6:2015():. doi: 10.1136/bcr-2014-204511. Epub 2015 Jul 6 [PubMed PMID: 26150609]
Level 3 (low-level) evidenceCatalán-Coronado S, Parrado-Carrillo A, Nogués-Castell J, Rosinés-Fonoll J, Camós-Carreras A, Alcubierre R, Carrión-Donderis MT, Bernal-Morales C, Sánchez-Dalmau B. Case report: Bilateral optic nerve sheath meningocele: clinical aspects. Frontiers in ophthalmology. 2024:4():1385485. doi: 10.3389/fopht.2024.1385485. Epub 2024 May 8 [PubMed PMID: 38984125]
Level 3 (low-level) evidence